 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
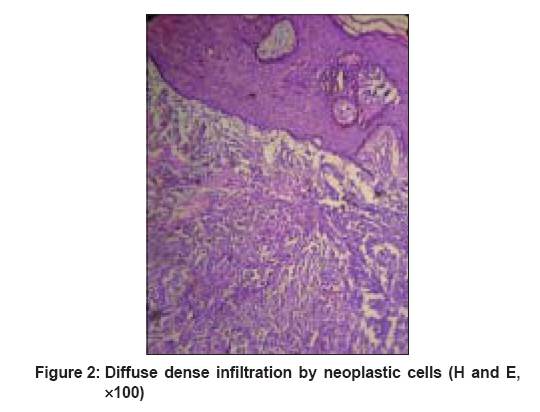
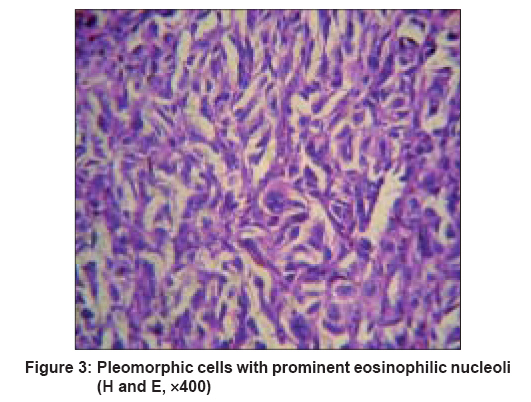
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 159-161 Letter To Editor Nodular melanoma in a skin graft site scar Rao AGnaneshwar, Jhamnani KamalK, Konda Chandana Department of Dermatology, Gandhi Medical College and Hospital, Musheerabad, Hyderabad Code Number: dv08061 Sir, Nodular melanoma is the second most common subtype of cutaneous melanomas with a frequency of 15-30%. [1] Most frequently it presents in midlife with a median age at presentation of 53 years, it is more common in males than in females. Recognition of nodular melanomas can be problematic as they lack many of the conventional clinical features. A 47 year-old man was referred to the Dermatology Department with complaints of a nonhealing ulcer over the right thigh and popliteal fossa prevalent since the last two years and also, nodules over the right lower limb extending up to the ankles observed for the last eight months. The patient was apparently asymptomatic two years before when he met with an accident leading to a nonhealing ulcer over the right thigh. There was no history of any burn injury. The ulcer was treated with skin grafting from the left thigh. The graft site healed well at that time. Gradually over the span of a few months, the patient developed small swellings over the scar of the grafted site. This was followed by ulceration and rapid growth of a fungating mass extending up to the popliteal fossa. This was associated with a serosanguineous discharge. Over the next year, the patient started developing skin-colored nodules over the right lower limb below the growth extending up to the dorsum of the foot. The growth was painless and asymptomatic to start with but as it grew, it caused pain and limitation of mobility due to pressure effects. The patient was otherwise well with no previous significant medical history. He was addicted to smoking and occasionally consumed alcohol. The general examination was unremarkable except for edema over the right foot. Cutaneous examination revealed a fungating mass over the right popliteal fossa with interspersed areas of necrosis and a healed ulcer over the lateral aspect of the thigh [Figure - 1]. Skin-colored to hyperpigmented nodules distributed over the entire right leg were firm to bony hard in consistency. Regional inguinal lymphadenopathy was present which was bony hard in consistency. With these features, a clinical diagnosis of Marjolin′s ulcer was made. Differential diagnoses that were considered included pigmented basal cell carcinoma, eccrine poroma, blue nevus and pyogenic granuloma. Skin biopsy was taken from the edge of the fungating mass and also from the nodule. Histopathological examination revealed extensive areas of necrosis, hemorrhage and tumor tissue with pleomorphic cells and pleomorphic nuclei with prominent eosinophilic nucleoli. Both intra- and extracellular melanin pigment was seen [Figure - 2],[Figure - 3]. The specimen revealed mitotic figures and also tumor giant cells. HMB-45 studies were positive. Based on these histopathological findings, a diagnosis of nodular melanoma was made. Malignant melanoma arising from burn scars are rare with only 27 cases being reported so far. [2] Malignant melanomas arising in skin grafts are even more rare with only two case reports. [3] Hall et al. reported a case who developed melanoma within a skin graft donor site and an invasive melanoma within the recipient graft site. [4] Carcinoma developing in burn scars is overwhelmingly of the squamous cell type. In fact, almost 2% of all squamous cell carcinomas develop in old burn scars. [5] According to recent literature, most of the melanomas have been reported in burn scars with an incidence of about 6% of all burn scar neoplasms. While reviewing 412 burn scar neoplasms, Kowal-Vern et al. reported a mean latency interval of 31 years. [6] The case under study had a latency interval of two years, which is short. Multiple malignant melanomas may develop in different burn scar areas. Hwang et al. described a case who developed malignant melanomas at two different sites of burn scars [7] Spring et al. have reported a case where malignant melanoma developed at the site of excision of a squamous cell carcinoma. [8] Gamatsi et al. have reported a case of malignant melanoma which developed in a burn injury treated with a skin graft. While analyzing the cause of malignant melanoma in grafted skin, the authors opined that the malignant melanoma might have been transferred to the recipient site along with the skin graft. [9] In view of varied clinical presentation of nodular melanoma, a high index of suspicion is needed in all cases of injuries and burns treated with skin grafts. Such cases need to be followed up periodically so that an early diagnosis can be made and treated promptly. We have presented this uncommon case to emphasize the importance of follow-up in cases of injury and burns treated with skin grafts. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08061f1.jpg] [dv08061f2.jpg] [dv08061f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}