 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
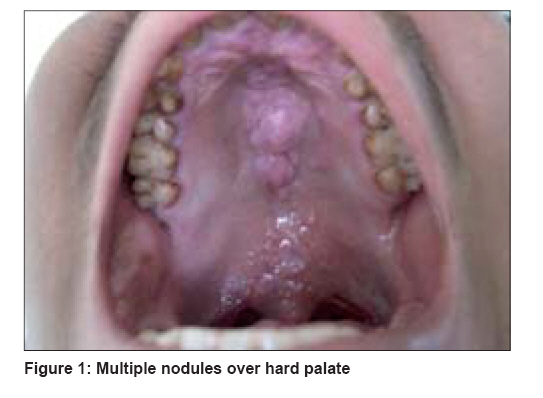
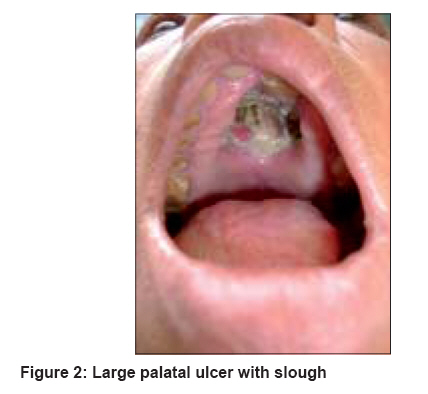
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 161-162 Letter To Editor Palatal involvement in lepromatous leprosy Rao AGnaneshwar, Konda Chandana, Jhamnani Kamal Department of Dermatology, Gandhi Medical College and Hospital, Secunderabad, Andhra Pradesh Code Number: dv08062 Sir, The involvement of the oral cavity is rare in leprosy. Lesions of the mouth and palate are usually found in patients of lepromatous leprosy and are more common in men than women. Various types of lesions observed are infiltration, ulceration, perforation and reddish yellow nodules. Oral and nasal lesions in leprosy are probably sources of the spread of bacilli and transmission of the disease as viable bacilli have been detected in these lesions. Here, we report two cases of lepromatous leprosy with palatal involvement. Our first case was a 21 year-old male who came to the Department of Dermatology with complaints of hypopigmented patches over the trunk prevalent since the last year and puffiness of face since the last three months associated with epistaxis, nasal stuffiness and change of voice. There was no positive family history of Hansen′s disease. General examination was normal except for the suffused face. Cutaneous examination revealed multiple, infiltrated, copper-colored plaques distributed on the face, trunk, arms and thighs. Ear lobes were infiltrated and two erythematous nodules were present on the left arm. Multiple, hypopigmented patches were distributed on the trunk, arms and thighs and sensations were decreased on the plaques and patches. Glove and stocking anesthesia was present and infraorbital, greater auricular, ulnar, lateral popliteal and posterior tibial nerves were thickened and tender on both sides. Examination of the oral cavity showed multiple nodules and plaques on the palate [Figure - 1]. With these clinical findings, a provisional diagnosis of lepromatous leprosy was made and the patient was subjected to investigations. Complete blood count, blood sugar, blood urea, liver function and renal function tests were within normal limits. Slit skin smears from both ear lobules showed bacterial loads of 6+. Skin biopsy showed atrophy of epidermis, subepidermal free grenz zone, inflammatory lesions around the adnexal structures and nerve bundles. Acid fast bacilli (AFB) stained sections showed packs of AFB(+) bacilli within the histiocytes (lepra cells). Biopsy taken from the plaque on the palate showed nonspecific changes. Our second case was a 50 year-old female who was brought to the department of dermatology with complaints of ulceration of the palate of six months′ duration. This was associated with pain while eating and nasal stuffiness and numbness of hands and feet. There was no positive family history for leprosy. General examination was normal except for wrinkling of face with ciliary and superciliary madarosis. Cutaneous examination revealed ichthyosis involving both the upper and lower limbs. Glove and stocking anesthesia was present. Both ulnar and lateral popliteal nerves were thickened and nontender. Examination of the oral cavity showed a large perforation of the palate measuring 4 cm x 2 cm covered with purulent, foul-smelling discharge and which was tender on palpation [Figure - 2]. A slit skin smear showed 5+ bacterial load. Skin biopsy showed features of lepromatous leprosy. A smear from the floor of the perforation did not reveal AFB bacilli. Biopsy from the palate showed features of nonspecific dermatitis. Involvement of the oral cavity in leprosy is less frequent than that of the nasal and nasopharyngeal cavities. Nevertheless, lesions of the mouth and palate are often found in patients of the Virchowian group. [1] Their prevalence has been reported to range from 19 to 60% among lepromatous leprosy patients. Oral lesions are more common in men than in women. In their studies, Reichart and Scheepers et al. found that more men than women have leprous oral lesions and that the palate was the most frequently affected location in the oral cavity. Various types of lesions observed are infiltration, ulceration, perforation, reddish or yellow reddish nodules, sessile or pedunculated, varying from 2 to 10 mm, some confluent and prone to ulceration. [2] The distribution of the oral lesions has been attributable to the preference of lepra bacilli to temperatures below 37°C. [3] Giridhar et al. and Brandt corroborate this, explaining the reasons for higher frequency of lesions in the palate′s midline. As the palate is a structure crossed by two air currents, the nasal and the oral, its temperature remains 1-2°C below the body temperature. [4] This may explain the location of the patient′s lesion on the palate midline. Oral and nasal lesions of leprosy are probably sources of the spread of bacilli and transmission of the disease as viable bacilli have been detected in these lesions by histopathological examination. Incidence of oral lesions is directly proportional to the distribution of the disease. Clinical features of the palate lesion in the male patient coincide with Reichart′s description that defines ′Hansenomas′ as reddish yellow, soft or hard, sessile, confluent lesions. No oral lesion can be clinically characteristic or pathognomonic of leprosy. The diagnosis is based on cutaneous lesions. Early diagnosis and antileprosy therapy prevents the occurrence of advanced and severe lesions. The differences in the progress of leprosy and the incidence of oral and facial lesions are also due to climatic, geographic and racial factors as well as the time of the disease onset and the duration of antileprosy therapy. [5] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08062f1.jpg] [dv08062f2.jpg] |
| |||||||||

{kind=link}
{kind=link}