 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
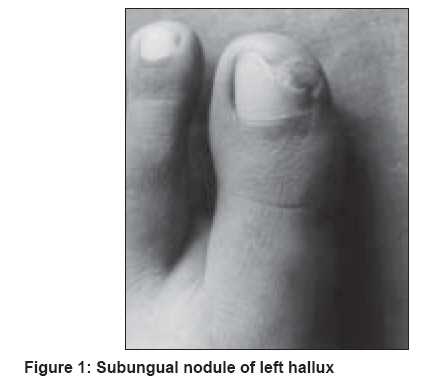
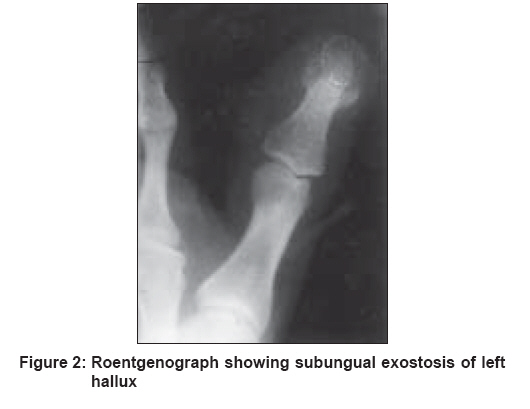
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 173-174 Letter To Editor Subungual exostosis Aggarwal Kamal, Gupta Sanjeev, Jain VijayKumar, Mital Amit, Gupta Sunita Department of Dermatology, Venereology and Leprology, M. M. Institute of Medical Sciences and Research, Mullana, Ambala Code Number: dv08073 Sir, A 27-year-old female presented with a slowly enlarging, slightly tender nodular growth under the medial border of the left hallucal nail. The duration of the lesion was roughly 3 years. Prior to that time, her big toes were normal in appearance. The patient did not recall any major or minor trauma affecting this nail. There was no history of chronic infection of the left big toe. The patient complained of mild pain in the distal part of the left big toe while walking. The nodular growth was well-defined in outline, firm in consistency, slightly tender and with a hyperkeratotic, smooth surface [Figure - 1]. It projected out beyond the free edge of the medial border of the left hallucal nail, causing elevation of the nail plate. A presumptive diagnosis of subungual wart was made, but repeated attempts at superficial paring of the topmost layer of the hyperkeratotic subungual area did not cause any improvement in the lesion. Radiographs of the foot [Figure - 2], taken at oblique angles and magnified, revealed an outgrowth of trabeculated bone projecting from the distal phalanx of the left big toe, on the dorsal aspect, with well-defined margins. There was no evidence of calcification of the soft tissues. No destructive changes were noted in the distal phalanx to suggest the possibility of a malignant lesion. This was interpreted as being consistent with the diagnosis of subungual exostosis. The patient underwent excision of the exostosis with satisfactory relief of symptoms. Histopathological study of the lesion was found to be consistent with the diagnosis of subungual exostosis. There has been no local recurrence after the patient underwent excision of the growth. Subungual exostosis may be defined as a solitary, benign tumor of bone occurring on the distal phalanx beneath the nail. [1] First described by Dupuytren in 1847, [2] it has not been much remarked on in the recent years. This peculiar tumor is relatively uncommon. [3] A solitary lesion most often occurs on the large toe [1] but also has occurred on the lesser toes and even on fingers. [4] A striking finding is the predilection for exostosis to occur on the inner border of the terminal phalanx of the large toe. Subungal exostosis usually develops during adolescence and is more common in females than males. The cause of subungual exostosis is unknown. Many factors have been suggested, including trauma, chronic infection, tumor, hereditary abnormality or activation of a cartilaginous cyst. [6] Initially, in typical cases, a small firm lesion appears, which is usually located deep to the free edge of the nail. Pain, particularly severe on walking, develops due to the collision of the nail plate with the expanding exostosis. The overlying nail is pushed up and is finally detached, leaving a mass of fibrous tissue whose surface may become eroded and infected. This mass overlies the exostosis. Differential diagnosis at this stage may include the following: subungual verruca, granuloma pyogenicum, glomus tumor, carcinoma of the nail bed, melanotic whitlow, keratoacanthoma, subungual epidermoid inclusions and enchondroma, K φenen′s tumor, keratocanthoma and ingrowing toe nail. [7] Since enchondroma, like an exostosis, may involve the distal portion of a phalanx and cause nail changes, it deserves a special mention. Roentgenographically, an exostosis is seen as a bony outgrowth from the phalangeal bone while radiolucent enchondroma causes expansion of the phalanx itself. Excision and curettage of the subungual exostosis is the treatment of choice. [7] The purpose of this article is to highlight the fact that, while examining subungual lesions, the possibility of subungual exostosis should be considered as it is often missed because X-ray films are routinely not advised for such type of lesions.[8] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08073f1.jpg] [dv08073f2.jpg] |
| |||||||||

{kind=link}
{kind=link}