
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 2, 2008, pp. 185-186
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 185-186
Quiz
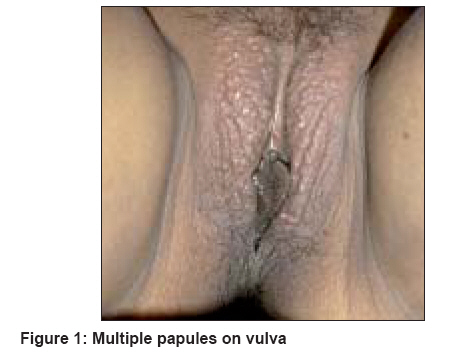
Multiple papules on the vulva
Rama Rao GRaghu, Rani RRadha, Amareswar A, Krishnam Raju PV, Kumari PRaja, Kumar YHari Kishan
Surya Skin Care and Research Center, Visakhapatnam
Correspondence
Address:Surya
Skin
Care
and
Research
Center,
#15-1-2,
Gopal
Sadan,
Naoroji
Road,
Maharanipeta,
Visakhapatnam
-
530
002,
Andhra
Pradesh,
graghuramarao@hotmail.com
Code Number: dv08077
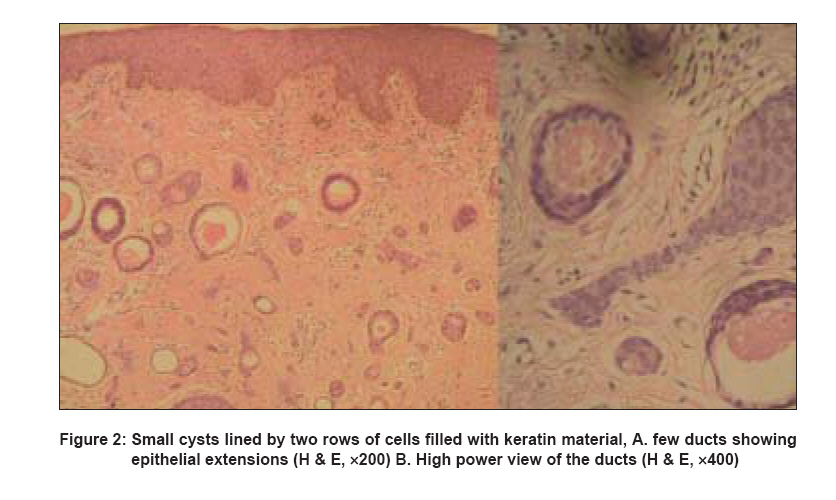
A 26 year-old married woman presented with a two-year history of asymptomatic, multiple papular lesions on the vulva. There was no history of premarital or extramarital exposure. On clinical examination, there were multiple, small, firm, skin-colored papules on the vulva [Figure - 1]. The lesions were nontender and there was no lymphadenopathy. Systemic examination including per vaginal and per rectum examinations, revealed no abnormality. Routine investigations were normal. Test for HBsAg, HIV I and II, VDRL were non-reactive. A 3 mm punch biopsy was done for the lesion. Histopathology showed a normal epidermis and the dermis showed a number of small cysts and ducts lined by two rows of cells. Some of the cysts were filled with keratin material. Walls of some of the ducts had epithelial extensions [Figure - 2].
What is your Diagnosis ?
DIAGNOSIS: SYRINGOMA OF THE VULVA
DISCUSSION
Syringoma is a benign tumor of eccrine sweat ducts
characterized by single or multiple, small, firm, skincolored
or yellowish papules. These papules have rounded
or flat-topped surfaces and may or may not be pruritic.
The most common site is the periorbital region (lower
eyelid); other areas are cheeks, axillae, abdomen and
genitals.[1]
Vulvar syringomas are rare with only a few cases reported in
literature.[2-6] They occur in young women after puberty.[2] The
most common presentation is that of multiple flesh-colored
or brownish papules on the labia majora. These lesions
are clinically difficult to differentiate from epidermal cysts,
steatocystoma multiplex, condyloma, Fox-Fordyce disease,
cherry hemangioma, angiokeratoma, soft fibroma and
lymphangioma circumscriptum.[7] They are one of the causes
for vulvar pruritus. Some patients have exacerbation of pruritus
and increase in the size of lesions during the summer or
during menstruation. A diagnosis of vulvar syringomas should
be considered if a patient with lichen simplex chronicus of
labia major responds poorly to oral antihistamine and topical
steroids.[2] Similarly, in men, syringomas can occur albeit rarely
on the penis.[6] A skin biopsy is necessary to confirm the
diagnosis.
No effective treatment modality has been documented.
Treatment options include excision, cryotherapy,
electrosurgery and carbon dioxide laser treatment. Topical
steroids and oral antihistamines were not effective in
controlling pruritus in our patient. Topical atropine and topical tretinoin may be tried.[8] Carbon dioxide laser is an effective therapeutic modality in patients with intractable
pruritus.[2]
Diagnosis : Syringoma of the Vulva
Discussion
Syringoma is a benign tumor of eccrine sweat ducts characterized by single or multiple, small, firm, skin-colored or yellowish papules. These papules have rounded or flat-topped surfaces and may or may not be pruritic. The most common site is the periorbital region (lower eyelid); other areas are cheeks, axillae, abdomen and genitals. [1]
Vulvar syringomas are rare with only a few cases reported in literature. [2],[3],[4],[5],[6] They occur in young women after puberty. [2] The most common presentation is that of multiple flesh-colored or brownish papules on the labia majora. These lesions are clinically difficult to differentiate from epidermal cysts, steatocystoma multiplex, condyloma, Fox-Fordyce disease, cherry hemangioma, angiokeratoma, soft fibroma and lymphangioma circumscriptum. [7] They are one of the causes for vulvar pruritus. Some patients have exacerbation of pruritus and increase in the size of lesions during the summer or during menstruation. A diagnosis of vulvar syringomas should be considered if a patient with lichen simplex chronicus of labia major responds poorly to oral antihistamine and topical steroids. [2] Similarly, in men, syringomas can occur albeit rarely on the penis. [6] A skin biopsy is necessary to confirm the diagnosis.
No
effective
treatment
modality
has
been
documented.
Treatment
options
include
excision,
cryotherapy,
electrosurgery
and
carbon
dioxide
laser
treatment.
Topical
steroids
and
oral
antihistamines
were
not
effective
in
controlling
pruritus
in
our
patient.
Topical
atropine
and
topical
tretinoin
may
be
tried. [8] Carbon
dioxide
laser
is
an
effective
therapeutic
modality
in
patients
with
intractable
pruritus. [2]
References
| 1. | Kaddu S, Kerl H. Appendage tumors of the Skin. Fitzpatrick's Dermatology in general medicine; 6 th ed. Vol. 1; McGraw - Hill Medical Publishers: p. 794-5. Back to cited text no. 1 |
| 2. | Haung YH, Chaung YH, Kuo TT. Vulvar syringoma: A clinico pathologic and immunohistologic study of 18 patients and results of treatment. J Am Acad Dermatol 2003;48:735-9. Back to cited text no. 2 |
| 3. | Tawade YV. Syringoma of the vulya. Indian J Dermatol Venereol Leprol 2000;66:326-7. Back to cited text no. 3 |
| 4. | Isaacson D, Turner ML. Localized vulvar syringomas. J Am Acad Dermatol 1979;1:352-6. Back to cited text no. 4 |
| 5. | Karam P, Benedetto AV. Syringomas: New approach to an old technique. Int J Dermatol 1996;35:219-20. Back to cited text no. 5 |
| 6. | Zalla SA, Perry HO. An unusual case of syringoma. Arch Dermatol 1971;103:215-7. Back to cited text no. 6 |
| 7. | Young AW Jr, Herman EW, Tovell HM. Syringoma of the vulva: Incidence, diagnosis and cause of pruritus. Obstet Gynaecol 1980;55:515-8. Back to cited text no. 7 |
| 8. | Klunger N, Mishra S, Jain RK, Saxena S, Multiple eccrine hidrocytomas: Report of two cases treated unsuccessfully with atropine ointment. Indian J Dermatol Venereol Leprol 2004;70:367-9. Back to cited text no. 8 |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08077f1.jpg]
[dv08077f2.jpg]
|

{kind=link}
{kind=link}