 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
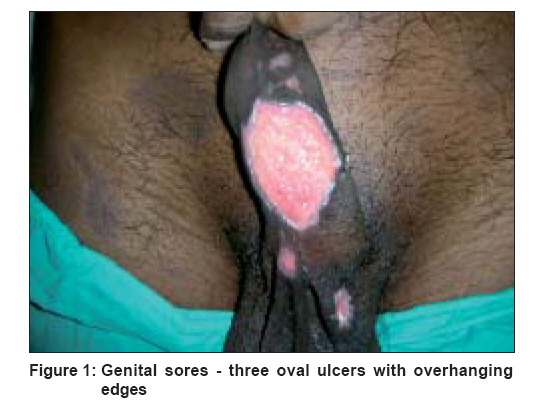
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 187 Net Case Cutaneous diphtheria masquerading as a sexually transmitted disease Vetrichevvel TP, Pise GajananA, Agrawal KishanKumar, Thappa DevinderMohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006 Code Number: dv08079 Abstract A 41 year-old, sexually promiscuous, married male, an agricultural laborer by occupation, presented to our sexually transmitted diseases (STD) clinic with multiple ulcers over the scrotum and genitalia of 20 days' duration. Bacterial culture from swabs taken from the genital ulcer, grew organisms morphologically and biochemically characteristic of Corynaebacterium diphtheriae. He made a complete and uneventful recovery after two weeks of therapy with antidiphtheria serum and crystalline penicillin. This case brings into light this hitherto unreported presentation of wound diphtheria mimicking a sexually transmitted genital ulcer disease and thus, underlines the importance of considering diphtheria as differential in atypical, long-standing genital ulcers. Keywords: Corynebacterium diphtheriae, Sexually transmitted disease, Wound Introduction Cutaneous diphtheria is becoming rare even in developing countries with the advent of proper immunization programs and better hygiene. [1] While there are five reports of genital diphtheria in the 1950s, there are no reports in the recent past. Here, we present a rare case of wound diphtheria masquerading as a sexually transmitted disease (STD).Case Report A 41 year-old married male, an agricultural laborer by occupation, presented to our STD clinic with multiple ulcers over the scrotum and genitalia of 20 days′ duration. He attributed the lesion to an episode of unprotected sexual exposure with an acquaintance, six weeks ago. There was no history of preceding vesicles over the genitalia or any systemic symptoms. On probing further, he revealed that the sexual exposure was followed by intense itching in the genitocrural region and that he had scratched the region leading to the formation of erosions. To contain the itching, he had taken a few oral native medications but with no effect, following which he had topically applied a paste made of crushed leaves over the region. After the application of the paste, the excoriations became deep and painful and started discharging clear fluid in the subsequent three weeks. Other than being thin in build, his general physical examination was unremarkable. On local examination, there were three well-defined, excavated, oval ulcers with overhanging edges; the floor showed pale-looking granulation tissue with clear serosanguineous discharge over the scrotum and the root of penis. The largest one measured 5.5 x 3.4 cm on the ventral aspect of the shaft of the penis [Figure - 1] along with ipsilateral, nontender, inguinal lymphadenopathy with lymph nodes each measuring about 2 x 1.5 cm in size. Multiple, small, healed erosions were also noted over the undersurface of the penis extending from the base to the tip of the penis. A differential diagnosis of donovanosis, syphilis and ulcerative herpes simplex virus infection with possible Human Immunodeficiency Virus (HIV) seropositivity was considered. The Tzanck smear, tissue smear and dark ground microscopy were negative, while Gram′s stain showed atypical, variably shaped, gram-positive organisms. Bacterial culture from swabs taken from the genital ulcer, grew organisms morphologically and biochemically characteristic of Corynebacterium diphtheriae which were susceptible to penicillin, erythromycin and vancomycin. Spot ELISA for HIV was negative and the culture from his throat swab ruled out a carrier state. He was isolated and treated with antidiphtheria serum (30,000 U intramuscularly) and crystalline penicillin two million units 6 th hourly intravenously. He made a complete and uneventful recovery after two weeks of therapy.Discussion Cutaneous diphtheria has three forms: (i) primary cutaneous diphtheria, which begins acutely as a tender pustular lesion, then breaks down and enlarges to form an oval, punched-out ulcer (ecthyma diphthericum) (ii) secondary infection on a preexisting wound (wound diphtheria) and (iii) superinfection of eczematized skin lesion. [2] Transmission of the infection occurs by contact with respiratory secretions, infected skin lesions and also by exposure to dust and fomites. Cutaneous diphtheria may be more contagious than respiratory diphtheria. [3],[4] Although myocarditis is relatively rare with cutaneous diphtheria, neurological complications including Guillain-Barrι syndrome can occur in 3-5% of ulcerated diphtheritic lesions. [5] Clinical suspicion of cutaneous diphtheria depends on epidemiological and morphological features. [6] These features include any kind of skin lesion in a patient with respiratory diphtheria, any form of diphtheria in the vicinity of a patient with skin lesions, slow-healing trauma of unprotected skin and recent travel to areas with epidemic diphtheria. Wound diphtheria occurs secondary to skin trauma (abrasions, lacerations, burns), chronic dermatitis, scabies and pyoderma and most commonly, involves the exposed areas of the feet, legs and hands, [3] while genital involvement is rare. A period of three weeks transpires between the primary lesion and evidence of superimposed diphtheria infection. In untreated, unimmunized patients, these ulcers may persist for as long as six months and the complications can occur as late as five months, hence, specific antitoxin (20,000-50,000 U intramuscular) should be administered if the diagnosis is suspected along with penicillin or erythromycin. This case brings into light this hitherto unreported presentation of wound diphtheria mimicking a sexually transmitted genital ulcer disease and thus, underlines the importance of considering diphtheria as a differential diagnosis in atypical, long-standing genital ulcers. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08079f1.jpg] |
| |||||||||

{kind=link}