 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
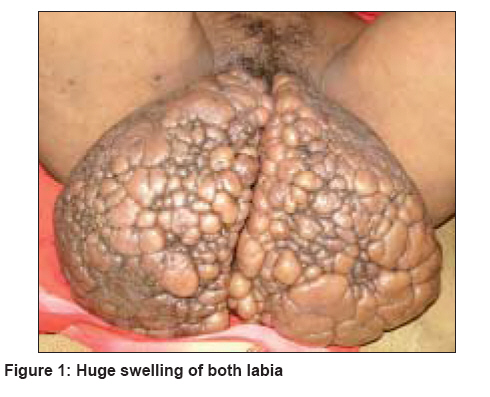
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 188 Net letter Cerebriform elephantiasis of the vulva following tuberculous lymphadenitis Nayak Surajit, Acharjya Basanti, Devi Basanti, Pattnaik Satyadarshi, Patra ManojKumar Department of Skin and VD, MKCG Medical College and Hospital, Berhampur Code Number: dv08081 Sir, Genital elephantiasis is an important medical problem in the tropics and usually affects the young and productive age group. Most reported cases occur as an end result of lymphatic obstruction due to various diseases like filariasis, Sexually Transmitted Diseases (STD) such as lymphogranuloma venereum (LGV) and donovanosis as well as malignancies. We report here a case of elephantiasis in a 35 year-old female. A 35 year-old woman, who had been married for 20 years, reported to the Skin and VD OPD of MKCG Medical College Hospital of Orissa, in the month of May 2007 with complaints of a genital swelling since the past 1.5 years. Her gait was unusually wide and on examination, we found a large, hypertrophied, pendulous, multilobed mass of hypertrophied tissue hanging down and obstructing the vulval cleft [Figure - 1]. The swelling was almost of the size of a human brain and comprised two separate parts which arose from both labia majora and were very symmetrical. The whole mass was pyriform in shape, firm and fibrosed, the surface was smooth, shiny and skin-colored with multiple lobular swellings of different sizes over it, resembling big pebble stones. The individual labial swelling was however, hemispherical with a medial vertical smooth surface apposed with the growth of the other side like that of an adult cerebral hemisphere. We could not visualize the introitus, clitoris and other parts due to the huge size of the swelling and the inability to introduce a speculum. No ulceration was seen on the surface. On examination, inguinal lymph nodes were palpable on both sides and they were matted, firm and nontender. Multiple puckered scars with overhanging margins were seen over both cervical and axillary regions of both sides without any sign of activity or discharge. Underlying lymph nodes in respective sites were small, fibrotic and nontender but matted, indicating old healed lesions. As stated by her, she had intermittent fever two years ago with marked weight loss for two months and subsequently, developed one discharging sinus over the left cervical region. She consulted a local physician and was given some antibiotic without any improvement. Subsequently, similar swellings appeared in the opposite side of the neck and axillae and a diagnosis of tubercular lymphadenitis was made. The patient was then discharged after being prescribed an antituberculosis regimen. She adhered to the regimen for the initial intensive phase, i.e. , two months at which the lesions healed and she discontinued the therapy without a single follow-up. After two months, she noticed signs of inflammation and swelling of both vulva without any pain but never reported to any doctor and the swellings gradually increased to attain the present size. But since the last few months, she again had low-grade fever with rapid loss of weight, for which she reported to us. The patient was a housewife with a single child. She and her spouse denied any extramarital exposure. No one in the family had any history of tuberculosis (TB). She was underweight (34 kg) and febrile. There was gross pallor and general physical and systemic examinations did not reveal any other abnormality. Vaginal, urethral and anal orifices appeared normal. Routine laboratory tests of urine and stool were normal. Hemoglobin was 8 gm%; total leukocyte count (TLC) 8600 cells/cubic mm; erythrocyte sedimentation rate (ESR) 80 mm at the end of first hour; Tridot screening for Human Immunodeficiency Virus (HIV), VDRL and serological tests for other STDs were negative. The night blood for microfilaria was negative. Mantoux test was strongly positive with blister formation [Figure - 2]. Sputum sample and fine needle aspiration cytology (FNAC) from inguinal lymph node was negative for acid-fast bacilli. X-rays of the chest and pelvic region were normal. A lymph node biopsy showed multiple granulomas comprising epithelioid cells, Langhans giant cells and lymphocytes, some showing central caseation necrosis. An ultra-sonogram of the pelvis was advised which showed fibrosed, atrophic, superficial inguinal lymph nodes. The patient did not allow for biopsy from the vulvar mass. Other biochemical parameters were within the normal range. A provisional diagnosis of relapsing TB lymphadenitis was made and a presumptive trial of antituberculosis therapy was initiated with a regimen of isoniazid 300 mg, rifampicin 450 mg, etambutol 800 mg and pyrazinamide 800 mg for the 1st two months and followed up with first two drugs for the following four months. After five weeks, there was symptomatic improvement and the patient was without fever and had started gaining weight. Taking into consideration the clinical features, histopathological findings, positive Mantoux and excellent therapeutic response, a confirmed diagnosis of resurgent tuberculous adenitis was made. However, the vulval lesion did not show any response. The patient was advised to complete the regimen and was further scheduled for a vulvectomy by a plastic surgeon after completion of therapy. Genital elephantiasis is defined as grotesque enlargement of the genitals due to lymphatic channel obstruction from various causes. Although the term ′elephantiasis′ was originally used to describe the elephant-like appearance of the legs, the term was subsequently used to describe the similar enlargement of the arm, chest, breast, penis, scrotum and vulva. [1] The term "esthiomene" is applied when genital elephantiasis is associated with ulceration in genital labia in females [3],[4] and is derived from a Greek verb, which means " to eat" and evoking the idea of something being gnawed, eroded or ulcerated. [5] The majority of the cases are due to filariasis; however, a small but significant proportion of patients develop genital elephantiasis due to bacterial sexually transmitted infections (STIs), mainly lymphogranuloma venereum (LGV) and donovanosis. STI-related genital elephantiasis should be differentiated from elephantiasis due to other causes, including filariasis, tuberculosis, hematological malignancies, iatrogenic or dermatological diseases. [6] Irrespective of etiology, the basic process remains the same, i.e. , permanent obstruction of lymphatic channels → lymphatic stasis → stimulation of growth of fibroblasts → destruction of lymph nodes → lymphedema and elephantiasis. In a patient with genital elephantiasis, the importance of taking proper history and thorough clinical examination cannot be overemphasized as it may help to find the cause for the elephantiasis. Rarely, genital elephantiasis has also been described as a complication of syphilis and infection with nonLGV strains of C. trachomatis. Laboratory investigations like microscopy of tissue smear and nucleic acid amplification test for donovanosis and serology and polymerase chain reaction for LGV may help in the diagnosis. However, in the absence of laboratory facilities in endemic areas, diagnosis largely depends on clinical characteristics. Elephantiasis associated with tuberculosis, closely resembles elephantiasis due to LGV, as both are associated with inguinal lymphadenitis. However, a reactive Mantoux test, suggestive histopathology, isolation of Mycobacterium tuberculosis by polymerase chain reaction (PCR) or culture and response to antituberculosis therapy are confirmatory for tuberculosis. [7],[8] In the context of tuberculosis, it must be remembered that the disease can also produce pseudoelephantiasis ( i.e. , elephantiasis of genitalia secondary to genital pathology) with a similar clinical presentation. [9],[10] Genital elephantiasis is a significant medical problem and persons affected may become a major burden to their family and community, especially when the disease interferes with their economic livelihood. At present, surgery is the only effective option for patients like this one, in whom the disorder is disabling, persistent and psychologically devastating. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08081f1.jpg] [dv08081f2.jpg] |
| |||||||||

{kind=link}
{kind=link}