
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 3, 2008, pp. 189-192
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 189-192
Editorial
Early antiretroviral therapy: The pendulum shifts again
Saple DG, Jindal Saurabh, Vaidya Satish
Department of Dermatology, Venereology and Leprology, GT Hospital and Grant Medical College, Mumbai
Correspondence Address:Department of Dermatology, Venereology and Leprology, GT Hospital, Mumbai
drsaple@gmail.com
Code Number: dv08084
Since the advent of highly active antiretroviral (HAART) in the mid-90s, the unequivocal benefit demonstrated by it in AIDS patients raised the question of the best time to initiate therapy. [1] Gradually, over the years, in response to increasing data, treatment schedules have changed from nucleoside reverse transcriptase inhibitors (NRTI) monotherapy to dual NRTI-based antiretroviral (ART) therapy and, most recently, to HAART. [2],[3] The euphoria over the efficacy of treatment initially led to a ′hit early-hit hard′ [4] approach, which favored initiation of ART when the CD4 count decreased to less than 500 cells/cu mm or the plasma HIV RNA level rose to above 30,000 copies/ml. [5] This initial enthusiasm started waning as awareness increased about the adverse effects of drugs, drug resistance, and the possibility of a persistent viral reservoir, leading to a more conservative approach. [6]
However, with new insights into disease pathogenesis - including the potential correlation of nadir CD4 cell count with clinical outcomes - and the introduction of newer antiretroviral agents, the pendulum appears to have swung back in favor of a more aggressive approach, with earlier initiation of HAART.
Rationale for Early Art Most of the lymphoid tissue of our body is located in the gut, and this tissue is infected early in HIV disease. A massive depletion of CD4 T-cells in the gut can be seen within weeks of infection; this persists throughout the chronic phase of infection and is rarely restored by ART. [7] Damage to gut mucosa enables translocation of microbial products such as lipopolysaccharides from the gut to the bloodstream, leading to ′switching on′ of the immune system and chronic immune activation. [8] The sustained fall in CD4 cell counts in HIV could be related to this chronic immune activation. Early treatment could potentially prevent the damage that may occur during this phase of clinical latency.
Pros of Early Art
According to the Department of Health and Human Services (DHHS) guidelines, the potential benefits of early treatment include the following: [9]
- Maintenance of a higher CD4+ cell count and prevention of potentially irreversible damage to the immune system
- Decreased risk for HIV-associated complications that can sometimes occur at CD4+ cell counts> 350 cells/cu mm; these complications include tuberculosis, non-Hodgkin′s lymphoma, Kaposi′s sarcoma, peripheral neuropathy, human papilloma virus-associated malignancies, and HIV-associated cognitive impairment
- Decreased risk of nonopportunistic conditions, including cardiovascular, renal, and liver disease, and non-AIDS-associated malignancies and infections
- Decreased risk of HIV-1 transmission to others
Maintenance of a higher CD4+ cell count and prevention of potentially irreversible damage to the immune system
There are various studies supporting this possibility. A recent analysis in the UK Collaborative HIV Cohort Study (CHIC) revealed that the cumulative increase in CD4+ cell count was dependent on the baseline CD4+ cell count, and only those patients who initiated therapy with nadir CD4+ cell counts> 350 cells/cu mm achieved eventual CD4+ cell counts similar - but not equal - to those observed in HIV-negative patients. [10] Similarly, data from the HOPS (HIV Outpatient Study) showed that there was a clear benefit in starting early ART in patients with CD4 < 500 cells/cu mm. [11] Data from the AIDS Therapy Evaluation Project, Netherlands (ATHENA), have also demonstrated that patients who started therapy at CD4 T-cell counts > 350 cells/cu mm were significantly more likely to achieve CD4 T-cell counts> 800 cells/cu mm after 7 years of therapy than those who initiated therapy at lower CD4 T-cell counts. [12]
Decreased morbidity and mortality
Studies on various cohorts have reported advantages in terms of decreased morbidity and mortality with early ART. In a large ′megacohort′ of 12 large HIV cohorts, Sterne and colleagues assessed the likelihood of HIV disease progression among 10,855 people and concluded that those who started HAART with CD4 cell counts < 200 cells/ mm 3 had a 3.68 times higher risk of AIDS as compared with those starting HAART with CD4 cell counts of 201-350 cells/ mm 3 . [13] Data from the ART Cohort Collaboration revealed that the risk for AIDS/death was significantly less in those who started therapy with a CD4 T-cell count between 200-350 mm 3 as compared with those who initiated ART at a CD4 threshold of 200 cells/mm 3 . [14] According to a new study from UK presented at the 15 th Conference on Retroviruses and Opportunistic Infections (CROI), 2008, patients with a CD4 cell count of 350 cells/mm 3 have more HIV related illnesses and a greater risk of death than patients with CD4 cell count more than 500 cells/mm 3 .
Lower risk of virologic failure and possible decrease in the risk of HIV transmission
Cozzi et al . found that patients starting HAART with a CD4 cell count < 200 cells/mm 3 tended to have a higher risk of subsequent virological failure as compared with patients with CD4> 350 cells/mm 3 . [15] Effective ART decreases infectious HIV RNA in many body reservoirs and is also likely to decrease transmission risk. Quinn et al . showed that viral load is the chief predictor of the risk of heterosexual transmission of HIV-1, and transmission is rare among persons with levels of less than 1500 copies of HIV-1 RNA per milliliter. [16] For example, in Taiwan, there was a decrease in HIV transmission after the introduction of a policy providing free access to ART, despite the fact that there was no change in sexual behavior (as assessed by examining the incidence of syphilis). [17] The decreased short-term risk for transmission afforded by effective ART may however be offset by the increased rates of high-risk behavior that have been reported in some settings. [18]
Reduced risk of serious non-AIDS conditions
Early clues to the existence of important non-AIDS HIV disease came from the Data Collection on Adverse Events of Anti-HIV Drugs (DAD) study, in which increasing rates of cancer and heart, liver, and renal disease were observed in HIV-infected persons as their CD4+ cell counts fell below 500 cells/mm 3 . [19] Several large observational studies have since indicated the same thing. [20],[21],[22] At CD4 counts> 200 cells/ mm 3 , HIV infected persons are more likely to die due to these non-AIDS serious illnesses, thus explaining the need for early ART.
Reduced risk of immune response inflammatory syndrome (IRIS)
IRIS is a major clinical problem when effective ART is started and poses a significant obstacle to achieving better outcomes when initiating therapy. Numerous studies have indicated that the risk for IRIS is linked to the CD4+ cell count at the time of initiating ART, with the highest risk observed when this the CD4+ cell count is < 50 cells/mm 3 . [23] Therefore, starting ART at higher CD4+ cell counts is likely to diminish the risk of IRIS.
Newer agents - simpler, less toxic, and more forgiving
The antiretroviral agent-related factors, including the impact of adherence to treatment, the adverse-effect profiles of the drugs, dietary restrictions necessary with the drug administration, and pill burdens, had a major bearing on the decision to defer initiation of ART. Newer antiretroviral agents have overcome many of these constraints and have resulted in improved compliance with treatment. This was achieved by allowing convenient dosing with minimal dietary restrictions by pharmacokinetic and formulation manipulations to reduce pill burden, and co-formulated dosage forms that contain two or three drugs in a single pill. Other improvements include the increased potency and longer half-lives of the newer agents, higher genetic barrier to resistance, efficacy against highly resistant strains, improved adverse-effect profile (e.g., less gastrointestinal effects, lesser impact on lipid profiles), as well as protease inhibitor boosting with ritonavir, which takes advantage of the potent cytochrome P450 inhibitory action of ritonavir. The newer agents also appear to be more ′forgiving′ in cases of missed doses. All these developments have together overcome the earlier negatives and now support earlier initiation of HAART. [24],[25],[26]
Cons of Early Art
Although there are more pros than cons for starting ART early it is probably prudent to recollect the negative consequences of early initiation of ART as they are probably more relevant to India than anywhere else. The potential risks of early treatment include:
- Development of treatment-associated adverse effects and toxicities
- Development of drug resistance due to incomplete viral suppression, resulting in loss of future treatment options
- These resistant strains may be further transmitted in the community with potentially disastrous consequences
- Increased total time on medication, with greater chance of treatment fatigue.
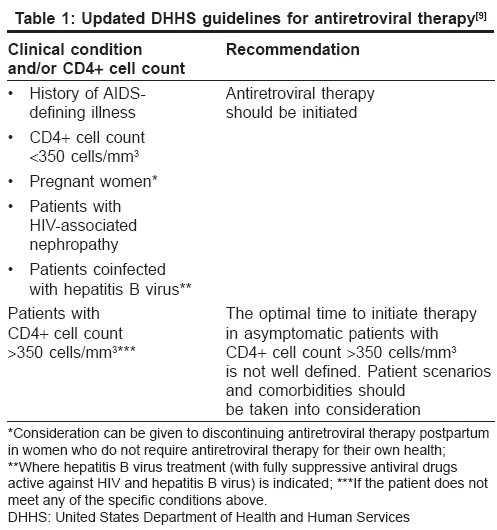
Current Recommendations Compared with the International AIDS Society-USA guidelines, [27] British HIV Association guidelines, [28] World Health Organization guidelines, [29] and NACO guidelines, [30] the updated DHHS guidelines [Table - 1] represent a modest shift towards earlier use of antiretroviral therapy. The recently updated European AIDS Clinical Society antiretroviral guidelines have CD4 thresholds for starting therapy similar to the updated DHHS guidelines, suggesting an evolving consensus on the topic. [31]
Conclusion
With continuing research in the field of HIV infection, expert opinion as to when to start ART for patients with CD4 < 350 cells/mm 3 has shifted back and forth for years; it is now close to reaching a consensus. The question which now remains is: At what level above 350 should ART be started? There have been no randomized clinical trials addressing this question. However, one study could provide some of the answers: The INSIGHT Network START Trial (Strategic Timing of Antiretroviral Therapy) is a randomized controlled trial of immediate vs deferred treatment for those with CD4 counts above 500 cells/mm 3 (START 500) and above 350 cells/mm 3 (START 350). This early treatment trial would focus on the impact of ART on the incidence of serious non-AIDS disease as well as traditional opportunistic diseases in patients with CD4+ counts that exceed current treatment guideline thresholds.
Ultimately, the patient is pivotal for arriving at the final decision to start ART. In addition to the patient′s CD4 cell count, other factors that are important in deciding whether to start ART include the rate at which the CD4 cell count changes over time, the plasma HIV RNA level, the clinical status, the presence of comorbidities, age, the patient′s readiness to begin therapy, the potential impact of ART on quality of life, and the likelihood of a high level of adherence to treatment. [9] The authors are of the opinion that in a resource-poor setting like ours, early ART initiation could potentially decrease the burden of opportunistic infections like tuberculosis in the country and thus become cost-effective in the long term.
One crucial aspect of any debate about when to start ART involves the capacity of the healthcare system to provide uninterrupted access to both care and drugs. Till that time physicians may wish to at least discuss the benefits of earlier initiation of ART with their patients.
References
| 1. | Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection: HIV Outpatient Study Investigators. N Engl J Med 1998;338:853-60. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Volberding PA, Lagakos SW, Koch MA, Pettinelli C, Myers MW, Booth DK, et al. Zidovudine in asymptomatic human immunodeficiency virus infection: A controlled trial in persons with fewer than 500 CD4-positive cells per cubic millimeter. N Engl J Med 1990;322:941-9. Back to cited text no. 2 [PUBMED] |
| 3. | Hammer SM, Katzenstein DA, Hughes MD, Gundacker H, Schooley R, Haubrich RH, et al. A trial comparing nucleoside monotherapy with combination therapy in HIV-infected adults with CD4 cell counts from 200 to 500 per cubic millimeter. N Engl J Med 1996;335:1081-90. Back to cited text no. 3 |
| 4. | Ho DD. Time to hit HIV, early and hard. N Engl J Med 1995;333:450-1. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Carpenter CJ, Fischl MA, Hammer SM, Hirsch MS, Jacobsen DM, Katzenstein DA, et al. Antiretroviral therapy for HIV infection in 1996. Recommendations of an international panel: International AIDS Society-USA Panel. JAMA 1996;276:146-54. Back to cited text no. 5 |
| 6. | Henry K. The case for more cautious, patient-focused antiretroviral therapy. Ann Intern Med 2000;132:306-11. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Haynes BP. Gut microbes out of control in HIV infection. Nat Med 2006;12:1351-2. Back to cited text no. 7 |
| 8. | Brenchley JM, Price DA, Schacker TW, Asher TE, Silvestri G, Rao S, et al. Microbial translocation is a cause of systemic immune activation in chronic HIV infection. Nat Med 2006;12:1365-71. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. January 29, 2008. p. 1-128. Available from: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. [last accessed on 2008 Mar]. Back to cited text no. 9 |
| 10. | Hughes R, Sabin C, Sterne J. Long-term Trends in CD4 Count in Patients Starting HAART: UK-CHIC Study [Abstract P18.4/04] 11 th European AIDS Conference, Madrid: 2007. Back to cited text no. 10 |
| 11. | Moorman AC, Holmberg SD, Marlowe SI, Von Bargen JC, Yangco BG, Palella FJ, et al. Changing conditions and treatments in a dynamic cohort of ambulatory HIV patients: The HIV outpatient study (HOPS). Ann Epidemiol 1999;9:349-57. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Gras L, Kesselring AM, Griffin JT, van Sighem, AI Fraser C, Ghani A, et al. CD4 cell counts of 800 cells mm 3 or greater after 7 years of highly active antiretroviral therapy are feasible in most patients starting with 350 cells, mm' or greater. J Acquir Immune Defic Syndr 2007;45:183-92. Back to cited text no. 12 |
| 13. | Sterne J, May M, Costagliola D, Egger M, Hogg R, Monforte AA, et al. Estimating the optimum CD4 threshold for starting HAART in antiretroviral-naοve HIV-infected individuals: Program and abstracts of the 13 th Conference on Retroviruses and Opportunistic Infections. Denver, CO: February 5-8, 2006. Back to cited text no. 13 |
| 14. | May M, Sterne JA, Sabin C, Costagliola D, Justice AC, Thiιbaut R, et al. Prognosis of HIV-1-infected patients up to 5 years after initiation of HAART: Collaborative analysis of prospective studies. AIDS 2007;21:1185-97. Back to cited text no. 14 |
| 15. | Cozzi Lepri A, Phillips AN, d'Arminio Monforte A, Castelli F, Antinori A, de Luca A, et al. When to start highly active antiretroviral therapy in chronically HIV-infected patients: Evidence from the ICONA study. AIDS 2001;15:983-90. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, Wabwire-Mangen F, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. N Engl J Med 2000;342:921-9. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Fang CT, Hsu HM, Twu SJ, Chen MY, Chang YY, Hwang JS, et al. Decreased HIV transmission after a policy of free access to highly active antiretroviral therapy in Taiwan. J Infect Dis 2004;190:879-85. Back to cited text no. 17 [PUBMED] [FULLTEXT] |
| 18. | Bezemer D, de Wolf F, Boerlijst M, Sighem A van, Hollingsworth D, et al. Despite HAART, HIV-1 is again spreading epidemically among men having sex with men in the Netherlands: Program and abstracts of the 14 th Conference on Retroviruses and Opportunistic Infections. Los Angeles, California: February 25-28, 2007. Back to cited text no. 18 |
| 19. | Weber R, Friis-Mψller N, Sabin CA, Reiss P, Monforte A, Dabis F, et al. HIV and non-HIV-related deaths and their relationship to immunodeficiency: The DAD study, Program and abstracts of the 12 th Conference on Retroviruses and Opportunistic Infections. Boston, Massachusetts: February 22-25, 2005. Back to cited text no. 19 |
| 20. | Weber R, Sabin CA, Friis-Moller N, Reiss P, El-Sadr WM, Kirk O, et al. Liver-related deaths 111 persons infected with the human immunodeficiency virus: The DAD study. Arch Intern Med 2006;166:1632-41. Back to cited text no. 20 |
| 21. | Patella FJ Jr, Baker RK, Moorman AC, Joan SC, Kathleen WC, John BT, et al. Mortality in the highly active antiretroviral therapy era: Changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr 2006;43:27-34. Back to cited text no. 21 |
| 22. | Lau B, Gauge SJ, Moore RD. Risk of non-AIDS-related mortality may exceed risk of AIDS-related mortality among individuals enrolling into care with CD4: Counts greater than 200 cells mm 3 . J Acquir Immune Defic Syndr 2007;44:179-87. Back to cited text no. 22 |
| 23. | French MA, Price P, Stone SF. Immune restoration disease after antiretroviral therapy. AIDS 2004;18:1615-27. Back to cited text no. 23 [PUBMED] [FULLTEXT] |
| 24. | Piacenti FJ. An update and review of antiretroviral therapy. Pharmacotherapy 2006;26:1111-33. Back to cited text no. 24 [PUBMED] [FULLTEXT] |
| 25. | Gallant JE. Should antiretroviral therapy be started earlier? Curr HIV/AIDS Rep 2007;4:53-9 Back to cited text no. 25 [PUBMED] |
| 26. | Shuter J. Forgiveness of non-adherence to HIV-1 antiretroviral therapy. J Antimicrob Chemother 2008;61:769-73. Back to cited text no. 26 [PUBMED] [FULLTEXT] |
| 27. | Hammer SM, Saag MS, Schechter M, Montaner JS, Schooley RT, Jacobsen DM, et al. Treatment for adult HIV infection: 2006 recommendations of the International AIDS Society-USA Panel. JAMA 2006;296:827-43. Back to cited text no. 27 [PUBMED] [FULLTEXT] |
| 28. | Gazzard B, Bernard AJ, Boffito M, Churchill D, Edwards S, Fisher N, et al. British HIV Association (BHIVA) guidelines for the treatment of HIV-infected adults with antiretroviral therapy (2006). HIV Med 2006;7:487-503. Back to cited text no. 28 [PUBMED] [FULLTEXT] |
| 29. | World Health Organization. Antiretroviral therapy for HIV infection in adults and adolescents: Recommendations for a public health approach. Available from: http://www.who.int/hiv/pub/guidelines/adult/en/index.html. [last accessed on 2008 Mar]. Back to cited text no. 29 |
| 30. | NACO Antiretroviral Therapy Guidelines for HIV-Infected Adults and Adolescents including Post-exposure Prophylaxis, May 2007. Back to cited text no. 30 |
| 31. | European AIDS Clinical Society (EACS) Guidelines for the Clinical Management and Treatment of HIV Infected Adults in Europe. Available from: http://www.eacs.eu/guide/1_Treatment_of_HIV_Infected_Adults.pdf. [last accessed 2008 Mar]. Back to cited text no. 31 |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08084t1.jpg]
|

{kind=link}