
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 3, 2008, pp. 200-207
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 200-207
Seminar: HIV Infection
Prevention of mother-to-child transmission
Surjushe Amar, Maniar Janak
Department of Dermatology, Venereology and Leprosy, Shri Vasantrao Naik Government Medical College, Yavatmal, Maharashtra
Correspondence Address:Department of Dermatology, Venereology and Leprosy, Shri Vasantrao Naik Government Medical College, Yavatmal, Maharashtra - 445 001
dramarsurjushe@rediffmail.com
Code Number: dv08087
Introduction
Mother-to-child transmission (MTCT) is the most important source of human immunodeficiency virus (HIV) infection in children below the age of 15 years. It affects approximately 5,00,000 infants per year all over the world and is responsible for 1800 new infections in children daily, the majority of which are in developing countries. The rate of perinatal transmission is 15-25% in developed countries, and 25-45% in developing countries. [1] In India, the Joint Technical Mission (2006) estimated that out of 27 million annual pregnancies, 189,000 occur in HIV-positive, pregnant women. An estimated cohort of 56,700 infected babies will be born annually in the absence of any intervention. The most affected states are Andhra Pradesh, Karnataka, Maharashtra, Tamil Nadu, and Manipur. [2]
In 1994, the Pediatric AIDS Clinical Trials Group (PACTG) protocol 076 reported a decrease in the risk of MTCT by nearly 70% due to the administration of zidovudine (AZT) to women from the fourteenth week of pregnancy onwards and during labour, and to the newborn in the absence of breastfeeding. [3] In non-breastfeeding populations, this regimen along with elective caesarean section decreased the transmission rate to ≤2%. [4],[5] Similar low vertical transmission has resulted with the use of highly active antiretroviral therapy by pregnant women. [6] Still in resource-poor settings, the limitations for these regimens are the cost and complexity. The regimens should be cost-effective, easily approachable, with high efficacy and should cause no or lesser side effects without any risk of resistance.
In developing countries like India, it was believed that husbands were mostly responsible for transmission of HIV in mothers through the sexual route and therefore, they are considered to be equally responsible for the transmission of HIV to their children. In India therefore, PMTCT is termed as PPTCT (prevention of parent-to-child transmission) so that mothers alone should not be blamed for HIV in their children. In India, the PPTCT program was started in 2002. Currently, there are more than 4000 Integrated Counselling and Testing Centres (ICTCs) in the country, most of these in government hospitals, which offer PPTCT services to pregnant women.
Rate of Transmission of HIV from Mother to Infant The rate of perinatal transmission without intervention is 19-36%. [7] Prenatal, intranatal and postnatal factors are responsible for MTCT. The rate varies in each scenario and these rates are important for the development of protective measures. Twenty-five to thirty-five per cent of total transmission occurs during the prenatal period, mainly in late pregnancy; [8] while 70-75% of total transmission occurs during the intranatal period. Postnatal transmission is via breast milk and accounts for 10-16% of all transmission. [9] The proposed mechanisms for intrapartum transmission are uterine contractions during labour that are responsible for micro-transfusion from constant massage of the placental bed and during labour exposure of the baby′s mucocutaneous surface to maternal blood and cervical secretions. As per the Pediatric Virology Committee of the AIDS Clinical Trials Group in the United States, a child with a positive PCR within 48 h of birth has been infected in utero and a child who is PCR-negative at 48 h but positive 7-90 days after delivery indicates an intrapartum infection. [10]
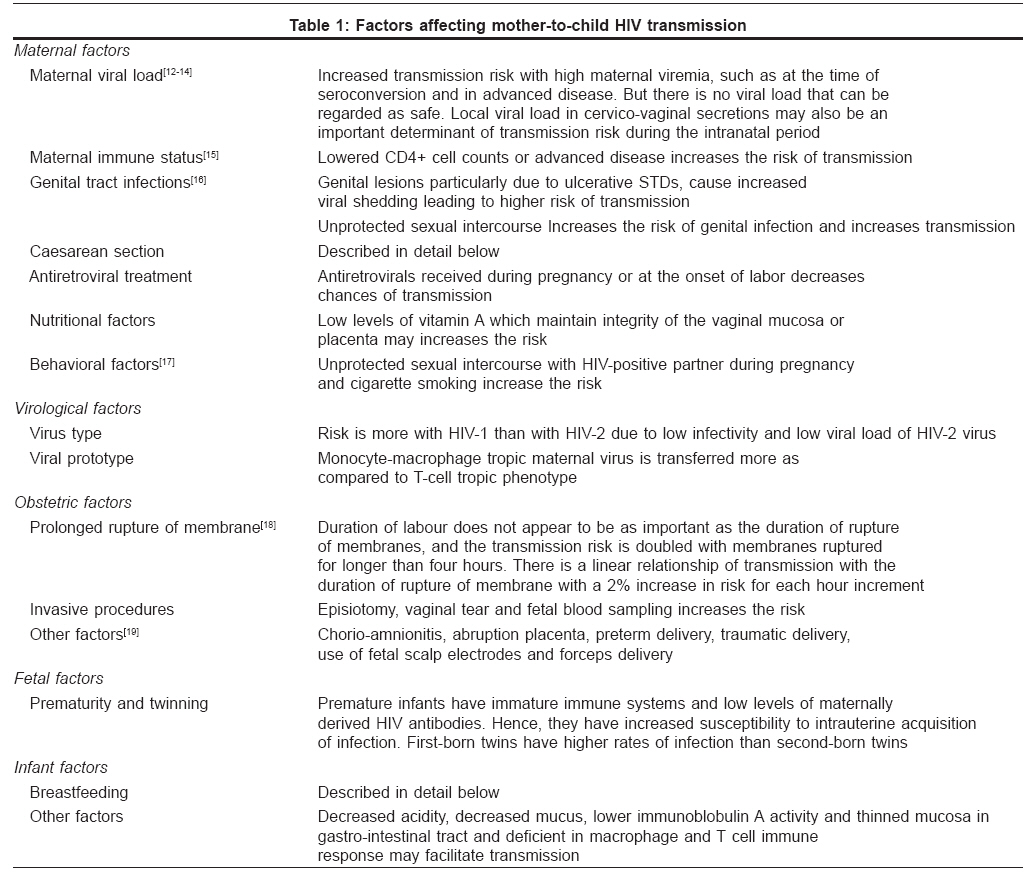
Factors Affecting Mother-to-Child HIV Transmission[1]
Mother-to-child transmission of HIV-1 is multifactorial. Factors responsible for mother-to-child can be divided into five categories: (1) maternal factors, (2) virological factors, (3) obstetric factors, (4) fetal factors and (5) infant factors [Table - 1]
Strategies for MTCT Prevention: [20]
The three-pronged approach to the prevention of MTCT is:
- Primary prevention of HIV among parents.
- Prevention of unwanted pregnancy in HIV-infected females
- Core interventions to prevent MTCT by HIV-positive mothers
Primary prevention of HIV infection includes HIV education; safe-sex practices; avoidance of intravenous drugs and sharing contaminated needles; prevention, diagnosis and early treatment of sexually transmitted diseases; change in moral behavior and attitude of the community. This is the only method that is 100% effective in preventing HIV transmission to infants.
Prevention of unwanted pregnancy in HIV-infected females, which is the most effective means of preventing MTCT, requires the provision of voluntary counseling testing (VCT) services and voluntary, safe, and effective contraception, sterilization, or pregnancy termination.
Core MTCT prevention intervention consists of compre-hensive maternal and child health services (antenatal, postnatal, and child health); voluntary counseling and testing (VCT), antiretroviral prophylaxis; counseling and support for safe infant feeding and optimal obstetrical practices. The major focus is on antiretroviral prophylaxis in this article.
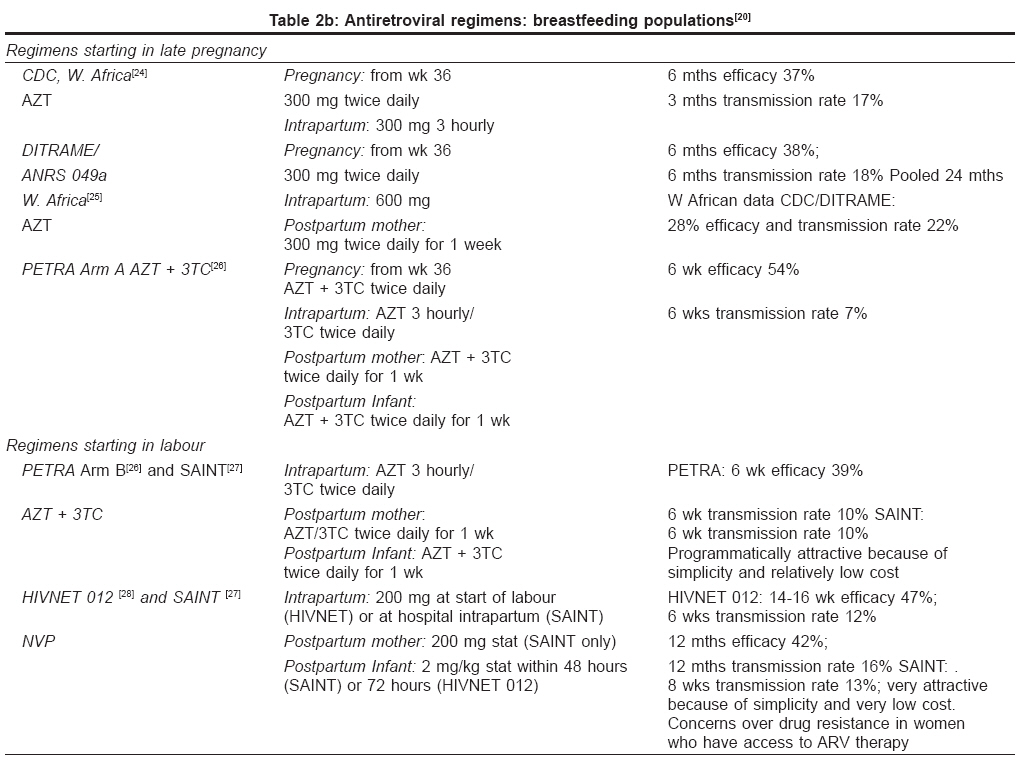
Antiretroviral regimens for prophylaxis
Due to the success of the Pediatric AIDS Clinical Trials Group (PACTG) protocol 076, various regimens have been developed [Table 2a] and [Table 2b]. In India, National AIDS Control Organization (NACO) has started to implement the single-dose-of-nevirapine (NVP) program in all the states beginning with the states with a high prevalence of HIV after the success of the HIVNET-012 study. [21] PPTCT services cover about 10% of the pregnancies in the country and 2.1 million pregnant women accessed this service in 2001. Of these, more than 16,500 pregnant women were HIV-positive.
Recommendations for use of antiretroviral prophylaxis in various clinical situations [29]
The following four scenarios should be considered while discussing HIV during pregnancy:
Scenario 1: HIV-1-infected pregnant women who have not received prior antiretroviral therapy: Recommendation
Standard clinical, immunological, and virological evaluation should be carried out. Recommendations for initiation and choice of antiretroviral therapy should be based on the same parameters used for persons who are not pregnant, although the known and unknown risks and benefits of such therapy given during pregnancy must be considered and discussed. If the viral load is> 1000 c (copies)/mL HAART including the three-part AZT regimen of PACTG 706, should be started. If the viral load is < 1000 c/mL, HAART or only AZT may be given according to the PACTG 706 protocol [Table 2a]. In the first trimester of pregnancy, one may consider delaying the initiation of therapy until after 10-12 weeks′ gestation because the risks associated with various agents taken during organogenesis are largely unknown. [30]
Scenario 2: HIV-1-infected women receiving antiretroviral therapy during the current pregnancy: Recommendation
Women receiving antiretroviral therapy and whose pregnancy is recognized during the first trimester, should be counseled regarding the benefits and potential risks of antiretroviral administration during this period, and continuation of therapy should be considered. Women receiving antiretroviral therapy and whose pregnancy is identified after the first trimester, should continue therapy. AZT should be a component of the antenatal antiretroviral treatment regimen after the first trimester whenever possible, although this may not always be feasible. [31] If therapy is discontinued during the first trimester, all drugs should be stopped and reintroduced simultaneously to avoid the development of drug resistance. [32] In case of NNRTI based regimen, stop NNRTI and continue NRTIs for 3-7 days so as to prevent drug resistance. Regardless of the antepartum antiretroviral regimen, AZT administration is recommended during the intrapartum period and for the newborn.
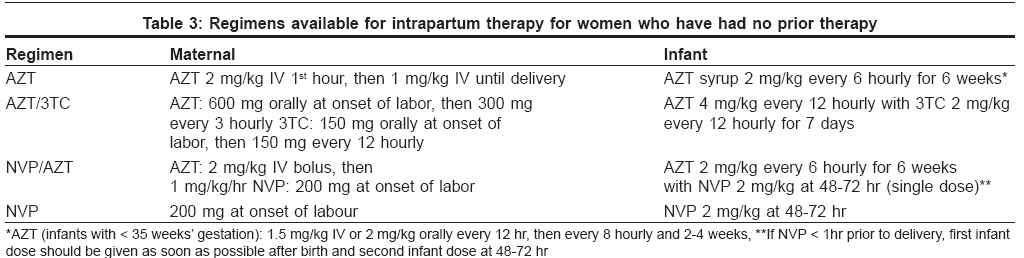
Scenario 3: HIV-1-infected women in labor who have had no prior therapy: Recommendation
Several effective regimens are available for intrapartum therapy for women who have had no prior therapy [Table - 3]. If single-dose nevirapine is given to the mother, alone or in combination with AZT, consideration should be given to adding maternal AZT/3TC starting as soon as possible (intrapartum or immediately postpartum) and continuing for 3-7 days, which may reduce the development of resistance to nevirapine. In order to plan continuation of therapy, the mother should have appropriate assessments ( e.g ., CD4+ cell counts and HIV1 RNA copy number) in the immediate postpartum period.
Scenario 4: Infants born to mothers who have received no antiretroviral therapy during pregnancy or intrapartum: Recommendation
AZT should be initiated as soon as possible after delivery, preferably within 6-12 hours of birth as per the ACTG 076 protocol. Some clinicians use AZT in combination with other ARV drugs, particularly if a mother is suspected of having an AZT-resistant virus. [33],[34] Efficacy for infants is currently unknown. In the immediate postpartum period, the mother should have appropriate assessments ( e.g ., CD4+ cell counts and HIV1 RNA copy number) to determine whether antiretroviral therapy is recommended for herself. Early HIV diagnostic testing should be done on infants so that if he or she is HIV-1 infected, treatment can be initiated as soon as possible.
Special issues related to the transmission of HIV from mother to child
Pre-conceptional counseling and care for HIV-1-infected women of childbearing age [35]
The Centers for Disease Control and Prevention (CDC), the American College of Obstetrics and Gynecology (ACOG), and other national organizations recommend offering preconception counseling and care as a component of routine primary medical care to all women of childbearing age. The purpose of preconception care is to improve the health of each woman prior to conception by identifying risk factors for adverse maternal or fetal outcome, providing education and counseling targeted to the patient′s individual needs, and treating or stabilizing medical conditions to optimize maternal and fetal outcomes.
Mode of delivery
Elective cesarean section (CS) at 38 weeks of pregnancy before the onset of labor or rupture of membrane decreases transmission by 50-80%. [36],[37] This transmission rate is further reduced to 2% when elective CS is combined with AZT prophylaxis. However, in mothers who have viral load < 1000 c/ml or have CS done after the onset of labor or rupture of membranes, there is no evidence of any benefit of CS in preventing perinatal transmission in fact, the risk of infectious complications increases 5-7 fold. So the decision of elective CS is based on the risk/benefit ratio.
Breastfeeding
The breast milk of HIV-infected mothers contains proviral HIV and free virus, as well as protective factors such as HIV antibodies and a glycoprotein that inhibits HIV binding to CD4+ cells. [38],[39] Despite the presence of these protective factors, a number of cases have been documented of transmission of HIV by breastfeeding. [40] The risk appears to be more during the first 4-6 months. [41] The risk of transmission is related to the duration of breast feeding, amount of virus in the breast milk, presence of HIV antibodies in the milk and whether or not breastfeeding is exclusive or mixed with other supplementary feeds. Mastitis, breast abscess, cracked nipples; infants with thrush, prolonged breastfeeding, and primary infection during pregnancy are other risk factors. In developed countries, breastfeeding is discouraged, however, in developing countries where formula puts the infant at high risk for other infections, breastfeeding is critical for infant nutrition and survival. [9]
Safety and adverse effects of antiretrovirals in pregnancy
Short-term safety and tolerance of antiretroviral prophylactic regimens has been demonstrated in all controlled clinical trials but data on long-term safety and on patterns of resistance is still being compiled. The following antiretrovirals should be avoided during pregnancy: Efavirenz (EFV), hydroxyurea, didanosine + stavudine (ddI + d4T), liquid amprenavir. [42] EFV causes neural tube defects in the first trimester while ddI + d4T causes severe lactic acidosis and/or hepatotoxicity. Nevirapine (NVP) causes fatal hepatic necrosis when given to pregnant women with CD4+ cells counts > 250/mm 3 , although it appears safe at delivery with only a concern for resistance with a single dose. Early pregnancy-associated nausea and vomiting may cause difficulty in antiretroviral administration or may exacerbate gastrointestinal side effects. Hyperglycemia and diabetes mellitus have been reported among patients taking protease inhibitors. [43]
Resistance
The frequency of NVP resistance is 60-70% with a single dose [44] with higher rates of NNRTI resistance mutations, especially K103N. In one trial, 15-24% of the mothers had NVP resistance six weeks postpartum with a single dose, which was no longer detected at 12 months. [45] But the probability that they were archived is supported by a lower rate of response to subsequent treatment with NVP-based HAART. [46] With AZT, development of resistance requires 4-6 months and AZT-resistant strains are infrequently transmitted. [47]
Conclusion
With the increase in pediatric HIV infection, there is a substantial impact on childhood mortality. MTCT not only increases the load of HIV-positive children on society, but also causes social problems by increasing the number of single parent-children or orphans after the death of one or both parents due to AIDS. Therefore, all pregnant women with HIV infection should be handled with utmost care, as there is a great potential of preventing HIV through vertical transmission. Antiretroviral prophylaxis either by combination therapy or a single agent, is recommended for all pregnant women with HIV-1 infection with careful and regular monitoring of the pregnancy and potential toxicities. In order to provide universal access to these services, further scale-up is planned up to the level of Community Health Centre and the Primary Health Centre, as well as in the private sector by forming public-private partnerships. Through these measures, NACO hopes to achieve the target of reducing the proportion of infants infected with HIV/AIDS by 50% by 2010. Still, the challenge for the future is to find the most cost-effective and feasible intervention to achieve 0% transmission of HIV from an infected mother to her child.
References
| 1. | Guidelines for the Prevention of Mother to Child Transmission of HIV. National AIDS Control Organisation. Available from: http://www.nacoonline.org/guidelines/guideline_9.pdf. Back to cited text no. 1 |
| 2. | World Health Organisation. (WHO) 2000a. Adaptation of the IMCI guidelines to take into account a high prevalence of HIV infection among children. Draft report of a consultative meeting in Durban, South Africa: August 16-18, 2000. Back to cited text no. 2 |
| 3. | Connor EM, Sperling RS, Gelber R, Kiseleve P, Scott G, O'Sullivan MJ, et al. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. N Engl J Med.1994;331:1173-1180. Back to cited text no. 3 |
| 4. | Kind C, Rudin C, Siegrist CA, Wyler CA, Biedermann K, Lauper U, et al. Prevention of vertical HIV transmission: Additive protective effect of elective Cesarean section and zidovudine prophylaxis. AIDS 1998;12:205-10. Back to cited text no. 4 |
| 5. | Mandelbrot L, Le Chenadec J, Berrebi A, Bongain A, Benifla JL, Delfraissy JF, et al. Perinatal HIV-1 transmission: Interaction between zidovudine prophylaxis and mode of delivery in the French Perinatal Cohort. JAMA 1998;280:55-60. Back to cited text no. 5 |
| 6. | Cooper ER, Charurat M, Burns DN, Blattner W, Hoff R. Trends in antiretroviral therapy and mother-infant transmission of HIV. J Acq Immune Defic Syndr 2000;24:45-7. Back to cited text no. 6 |
| 7. | Coutsoudis A, Pillay K, Kuhn L, Spooner E, Tsai WY, Coovadia HM. Method of feeding and transmission of HIV1 from mothers to children by 15 months of age: Prospective cohort study from Durban, South Africa. AIDS 2001;15:37987. Back to cited text no. 7 |
| 8. | Ehrnst A, Lindgren S, Dictor M. HIV in Pregnant Women and their Offspring: Evidence for Late Transmission. Lancet 1991;338:203-7. Back to cited text no. 8 |
| 9. | Nduati R, John G, Mbori-Ngacha D, Richardson B, Overbaugh J, Mwatha A, et al. Effect of breastfeeding and formula feeding on transmission of HIV-1: A randomized clinical trial. JAMA 2000;283:1167-74. Back to cited text no. 9 |
| 10. | Kapoor A, Kapoor A, Vani SN. Prevention of mother to child transmission of HIV. Indian J Pediatr 2004;71:247-51. Back to cited text no. 10 |
| 11. | Peckham C, Gibb D. Mother-to-child transmission of the human immunodeficiency virus. N Engl J Med 1995;333:298-302. Back to cited text no. 11 |
| 12. | Cao Y, Krogstad P, Korber BT, Koup RA, Muldoon M, Macken C, et al. Maternal HIV-1 viral load and vertical transmission of infection: The Ariel Project for the Prevention of HIV Transmission from mother to infant. Nat Med 1997;3:549-52. Back to cited text no. 12 |
| 13. | Garcia PM, Kalish LA, Pitt J, Minkoff H, Quinn TC, Burchett SK, et al. Maternal level of plasma HIV Type 1 RNA and the risk of Perinatal transmission. N Engl J Med 1999;341:394-402. Back to cited text no. 13 |
| 14. | Bailey A, Newell ML, Peckham C, De Rossi A, Ehrnst A, Grosch-W φmer I, et al. Maternal viral load and vertical transmission of HIV-1: An important factor but not the only one. AIDS 1999;13:1377-85. Back to cited text no. 14 |
| 15. | Natural history of vertically acquired human immunodeficiency virus-1 infection: The European Collaborative Study. Pediatrics 1994;94:815-9. Back to cited text no. 15 |
| 16. | Lee MJ, Hallmark HJ, Frankel LM, Del Priore G, Maternal Syphilis and Vertical Transmission of human immunodeficiency virus Type 1. Infect Int J Obstet Gynaecol 1998;63:247-52. Back to cited text no. 16 |
| 17. | Bulterys M, Landesman S, Burns DN, Rubinstein A, Goedert J. Sexual behavior and infection drug use during pregnancy and vertical transmission of HIV-1. J Acquir Immune Defic Syndr Hum Retrovirol 1997;15:76-82. Back to cited text no. 17 |
| 18. | Read J; for the Intl Perinatal HIV Group. Duration of rupture of membranes and vertical transmission of HIV-1: A meta-analysis from fifteen prospective cohort studies. 7 th Conf Retrovirus Opportunistic Infect (Abst 659), Jan 30-Feb 2, 2000. Back to cited text no. 18 |
| 19. | Goldenberg RL, Vermund SH, Goepfert AR, Andrews WW. Choriodecidual inflammation: A potentially preventable cause of Perinatal HIV-1 transmission. Lancet 1998;352:1927-30. Back to cited text no. 19 |
| 20. | Prevention of Mother-to-Child Transmission of HIV in Asia: Practical Guidance for Programs June 2002, Breastfeeding, LAM, Related Complementary Feeding, and Maternal Nutrition Program. Back to cited text no. 20 |
| 21. | Efficacy of Antiretroviral Regimens for the Prevention of Mother to Child Transmission of HIV and Some Programmatic Issues: Farley T, Buyse D, Gaillard P, Perriens J. Background documents for WHO Technical Consultation October 2000.1. Back to cited text no. 21 |
| 22. | Shaffer N, Chuachoowong R, Mock PA, Bhadrakom C, Siriwasin W, Young NL, et al. Short-course zidovudine for perinatal HIV-1 transmission in Bangkok, Thailand: A randomised controlled trial. Lancet 1999;353:773-80. Back to cited text no. 22 |
| 23. | Lallemant M, Jourdain G, LeCoeur S, Kim S, Koetsawang S, Comeau AM, et al. A trial of shortened Zidovudine regimens to prevent mother-to-child transmission of human immunodeficiency virus type 1. N Engl J Med 2000;343:982-91. Back to cited text no. 23 |
| 24. | Wiktor SZ, Ekpini E, Karon JM, Nkengason J, Maurice C, Severin ST, et al. Short course oral zidovudine for prevention of mother-to-child transmission of HIV-1 in Abidjan, C τte d'Ivoire: A randomised trial. Lancet 1999;353:781-5. Back to cited text no. 24 |
| 25. | Dabis F, Msellati P, Meda N, Welffens-Ekra C, You B, Manigart O, et al. 6-month efficacy, tolerance, and acceptability of a short regimen of oral zidovudine to reduce vertical transmission of HIV in breastfed children in C τte d'Ivoire and Burkina Faso: A double-blind placebo-controlled multicentre trial. DITRAME Study Group. Lancet 1999;353:786-92. Back to cited text no. 25 |
| 26. | Gray G. Early and late efficacy of three short ZDV/3TC combination regimens to prevent mother-to-child transmission of HIV-1, Abstract LbOr5, 13 th International AIDS Conference, Durban, South Africa, 9-14 July 2000. Back to cited text no. 26 |
| 27. | Moodley D; on behalf of the SAINT Investigators Team. The SAINT trial: Nevirapine (NVP) versus zidovudine (ZVD) + lamivudine (3TC) in prevention of peripartum HIV transmission. Abstract LbOr 2, 13 th International AIDS Conference 2000, Durban, South Africa. Back to cited text no. 27 |
| 28. | Guay LA, Musoke P, Fleming T, Bagenda D, Allen M, Nakabiito C, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomised trial. Lancet 1999;354:795-802. Back to cited text no. 28 |
| 29. | Public Health Service Task Force. Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV-1 Transmission in the United States Md: AIDSinfo, US Department of Health and Human Services; 2006. Available from http://www.aidsinfo.nih.gov/guidelines. [last accessed on 2006 Oct 12]. Back to cited text no. 29 |
| 30. | Garcia-Tejedor A, Perales A, Maiques V. Protease inhibitor treatment in HIV pregnant women: Is it safe for newborns? Int J Gynaecol Obstet 2002;76:175-6. Back to cited text no. 30 |
| 31. | Lambert JS, Watts DH, Mofenson L, Stiehm ER, Harris DR, Bethel J, et al. Risk factors for preterm birth, low birth weight, and intrauterine growth retardation in infants born to HIV-infected pregnant women receiving zidovudine. AIDS 2000;14:1389-99. Back to cited text no. 31 |
| 32. | Ioannidis JP, Abrams EJ, Ammann A, Bulterys M, Goedert JJ, Gray L, et al. Perinatal transmission of human immunodeficiency virus type 1 by pregnant women with RNA virus loads <1000 copies/mL. J Infect Dis 2001;183:539-45. Back to cited text no. 32 |
| 33. | Tuomala RE, Shapiro D, Mofenson LM, Bryson Y, Culnane M, Hughes MD, et al. Antiretroviral therapy during pregnancy and the risk of adverse outcome. N Engl J Med 2002;346:1863-70. Back to cited text no. 33 |
| 34. | Gray J. HIV in the neonate. J Hosp Infect 1997;37:181-98. Back to cited text no. 34 |
| 35. | American College of Obstetricians and Gynecologists. ACOG Committee Opinion number 313, September 2005. The importance of preconception care in the continuum of women's health care. Obstet Gynecol 2005;106:665-6. Back to cited text no. 35 |
| 36. | Elective cesarean section versus vaginal delivery in prevention of vertical HIV transmission: A randomized clinical trial. European Mode of Delivery Collaboration. Lancet 1999;353:1035-9. Back to cited text no. 36 |
| 37. | The mode of delivery and the risk of vertical transmission of human immunodeficiency virus type 1: A meta-analysis of 15 prospective cohort studies. N Engl J Med 1999;34:977-87. Back to cited text no. 37 |
| 38. | Wise J. Breast feeding safer than mixed feeding for babies of HIV mothers. Br Med J 2001;322:511-3. Back to cited text no. 38 |
| 39. | Newburg DS, Viscidi RP, Ruff A, Yolken RH. A human milk factor inhibits binding of human immunodeficiency virus to the CD4 receptor. Pediatr Res 1991;31:22-8. Back to cited text no. 39 |
| 40. | Stiehm ER, Vink P. Transmission of human immunodeficiency virus infection by breast-feeding. J Pediatr 1991;118:410-2. Back to cited text no. 40 |
| 41. | Miotti PG, Taha TE, Kumwenda NI, Broadhead R, Mtimayalye LA, Van der Hoeven L, et al. HIV transmission through breastfeeding: A study in Malawi. JAMA 1999;282:744. Back to cited text no. 41 |
| 42. | Watts DH. Management of human immunodeficiency virus infection in pregnancy. N Engl J Med 2002;346:1879-91. Back to cited text no. 42 |
| 43. | Visnegarwala F, Krause KL, Musher DM. Severe diabetes associated with protease inhibitor therapy. Ann Intern Med 1997;127:947. Back to cited text no. 43 |
| 44. | Flys T, Nissley DV, Claasen CW, Jones D, Shi C, Guay LA, et al. Sensitive drug-resistance assays reveal long-term persistence of HIV-1 variants with the K103N nevirapine (NVP) resistance mutation in some women and infants after the administration of single-dose NVP: HIVNET 012. J Infect Dis 2005;192:24. Back to cited text no. 44 |
| 45. | Cunningham CK, Chaix ML, Rekacewicz C, Britto P, Rouzioux C, Gelber RD, et al. Development of resistance mutations in women receiving standard antiretroviral therapy who received intrapartum nevirapine to prevent perinatal human immunodeficiency virus type 1 transmission: A substudy of the pediatric AIDS clinical trials group protocol 316. J Infect Dis 2002;186:181-8. Back to cited text no. 45 |
| 46. | Jourdain G, Ngo-Giang-Huong N, Le Coeur S, Bowonwatanuwong C, Kantipong P, Leechanachai P, et al. Perinatal HIV prevention trial group. Intrapartum exposure to nevirapine and subsequent maternal responses to nevirapine-based antiretroviral therapy. N Engl J Med 2004;351:229-40. Back to cited text no. 46 |
| 47. | Colgrove RC, Pitt J, Chung PH, Welles SL, Japour AJ. Selective vertical transmission of HIV-1 antiretroviral resistance mutations. AIDS 1998;12:2281-8. Back to cited text no. 47 |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08087t3.jpg]
[dv08087t2b.jpg]
[dv08087t2a.jpg]
[dv08087t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}