
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 3, 2008, pp. 208-214
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 208-214
Seminar: HIV Infection
Use of anti-retrovirals in pediatric HIV infection
Gaur Sunanda
Department of Pediatrics, Division of Allergy, Immunology, and Infectious Disease, UMDNJ/Robert Wood Johnson Medical School, New Brunswick, New Jersey
Correspondence Address:1 Robert Wood Johnson Place, MEB 322, New Brunswick, NJ 08901
gaursu@umdnj.edu
Code Number: dv08088
Introduction In resource-rich countries, the prognosis of pediatric HIV infection has undergone a dramatic transformation since the availability of antiretroviral drugs (ARV), particularly with the advent of highly active antiretroviral treatment regimens (HAART) in the later part of the 1990s. As a direct consequence of the availability and use of HAART, marked declines in mortality and morbidity have been reported in recent years. [1],[2],[3] While the general guiding principles governing the use of anti-retrovirals are similar in adults and children, there are several important differences and unique biological, as well as sociological features of pediatric HIV infection, which must be understood and appreciated in order to optimally treat HIV infection in children. The treatment of HIV in children is further challenging due to the relative paucity of palatable and effective drug formulations especially for the younger children. This is particularly problematic as increasing numbers of children acquire or develop drug-resistant viruses.
Unique Considerations in Pediatric HIV
- Virological Considerations: As the vast majority of children acquire HIV at or near the time of birth, most infants with HIV essentially develop primary HIV infection while they are immunologically immature and during a period of dramatic change in growth and neurological development. During this early period, the HIV RNA levels which are generally low at birth ( i.e., < 10,000 copies/mL), reach very high levels by two months of age (values ranging from undetectable to nearly ten million copies/mL) and then decrease slowly. The mean value in the first year is in the range of 185,000 copies/mL. [4] A very high RNA level (>299,000 copies/mL) in the first year of life has been correlated with disease progression and death. [5] However, contrary to what is seen in adults, RNA levels have demonstrated sufficient overlap between children who go on to develop disease progression and death and those who do not progress as rapidly. Thus, the predictive value of RNA levels in the first year of life remains modest. [4],[5] However, at any given level of viral load, untreated infants younger than a year-old, who have been diagnosed with HIV, are at a higher risk of disease progression and death. The predictive value is relatively improved in older children. [4],[5],[6]
- Immunological markers in children: In healthy, uninfected infants and children, the CD4 values have been known to be much higher than in uninfected adults. These values gradually decline with age to reach adult values by 4-6 years of age. [7] The percentage of CD4+ cells - a parameter that tends to show less age-related variability than CD4 counts - lends itself to more consistent monitoring. Age-based definitions for immune suppression have been formulated to provide guidance for the monitoring of disease progression in infants and children. The predictive value of the CD4+ cell percentage for disease progression varies with age. For any given CD4+ cell percentage, a child younger than one year old has a much greater risk of disease progression compared to an older child. In all ages however, a CD4+ cell percentage < 15% poses a greater risk of disease progression and death. [8] Overall, the ability to predict disease progression and death increases when both the CD4+ cell % and viral load values are considered together. [5],[6],[8]
- Neonatal exposure to zidovudine (ZDV) and other anti-retrovirals: Chemoprophylaxis and HIV treatment during pregnancy pose a unique risk for infants who develop HIV infection despite these strategies. Recent data have demonstrated that as many as 24% of (5/21) infants had drug-resistant virus prior to the initiation of antiretroviral treatment. [9] The majority of these infants harbored nonnucleoside reverse transcriptase inhibitor (NNRTI)-resistant virus primarily due to maternal chemoprophylaxis. This has important implications in the selection of antiretroviral regimens in infants as this reservoir of resistant virus has been shown to persist for up to 96 weeks. [9]
- Changes in pharmacokinetic parameters with age: It has long been recognized that the metabolism and pharmacodynamics of drugs vary in children with the growth and maturity of organ systems over time. Similarly, puberty has an impact on drug metabolism and clearance as well. [10] Traditional dictum has been that adolescents in early puberty (Tanner Stages I and II) can be prescribed medications using pediatric dosing guidelines, whereas adolescents in late puberty (Tanner stages IV and V) may be dosed using adult guidelines. In the case of HIV infection, few antiretrovirals have been studied in adolescents during pubertal phases to determine if this dictum applies. Additionally delayed puberty, which is frequently encountered in pediatric HIV, may pose further difficulties in dose recommendation. [11] Despite these issues, many of the antiretrovirals have not been fully studied. As of September 2005, of the 21 antiretrovirals approved by the US Food and Drug Administration for use in adults, only 13 were approved for use in children and only 11 had pediatric formulations. [12] Furthermore, the use of liquid formulations can pose barriers if their taste is not agreeable. Some liquids require large volumes to be dispensed or need refrigeration, which may also be a barrier in resource-poor settings. Appropriate and safe pediatric dosing necessitates weight- or surface area-based calculations that may also vary by age. Fixed dose combinations (FDCs) that are widely available for adults are not available for children. [12] Cutting or directly scaling down the adult FDCs is not a valid practice without appropriate pharmacokinetic studies and can lead to under- or overdosing of one or more components. [12] Breaking tablets to achieve pediatric dosing is not an optimal practice, especially for FDCs as it may lead to unequal dosing if the tablets are not formulated in equal layers.
- Adherence Issues: It is well recognized that maximal adherence to the prescribed ARV regimen is crucial for achieving and maintaining optimal antiretroviral response. [13],[14],[15] To achieve optimal adherence in growing children, a thorough and detailed evaluation of the family environment and caretakers′ attitudes and beliefs towards treatment and the ability to administer the prescribed regimen, needs to occur at the start of the treatment, and should be monitored at each visit during the entire treatment period. Any potential problems need to be resolved prior to treatment initiation even if this means that the treatment needs to be delayed. During early adolescence, a partnership with the child should be developed with the goal of providing disease education and empowerment regarding the need for medications and adherence. At this juncture, disclosure of HIV diagnosis to the child and to others in the child′s environment becomes a key factor. A nonjudgmental, trusting relationship between the teen and the provider is crucial at this stage. In addition, the recognition and management of the HIV-associated myriad of psychosocial and mental health issues is another important facet, which has a major impact on adherence, and must be addressed for successful management of HIV.
- Multidisciplinary team approach: Pediatric HIV is a multifaceted chronic illness with complex psychosocial ramifications. Economic, cultural, and psychological factors play a major role in the overall well-being of the infected child. As a result, an HIV-infected child must not be treated in isolation. It is crucial to address the emotional, mental, developmental, and nutritional needs of the child and the family. A team of individuals from various disciplines such as medical, nursing, social work, mental health, nutrition, and outreach workers need to work collaboratively to achieve the ideal results.
Initiating Antiretroviral Treatment
In general, the recommendations for antiretroviral therapy initiation are more aggressive in children as disease progression is known to occur more rapidly. As discussed earlier in this chapter, laboratory markers are less reliable predictors of disease progression in children (in particular in infants). Yet controversy exists among experts about whether to begin early treatment in asymptomatic children or to delay treatment initiation until evidence of disease progression and immunologic deterioration appears. Proponents of the "hit early, hit hard" concept of starting treatment without waiting for symptoms to appear, propose that early aggressive treatment allows for optimal viral suppression before the development of multiple ′quasispecies′ of HIV as a result of unchecked viral replication and preserves immune function. Advocates of delayed therapy point to better ARV adherence in symptomatic patients, preservation of antivirals for a later date and a delay in adverse effects since lifelong therapy may be needed. Regardless of which strategy is adopted, in individual instances, initiation of ARV is almost never an "urgent matter". Adherence to the chosen regimen is ultimately the most important determinant of success and achieving adherence requires in-depth assessment of the child and his/her family environment and the readiness of the caretaker to embark on treatment and all its inherent challenges. Time taken upfront to prepare the family unit for antiretrovirals is one of the most valuable and important aspects of initiating ARV.
Treatment of infants < 12 months old
This is due to data supporting the notion that infected infants younger than 12 months old are at a greater risk for disease progression and death and the fact that immunological and virological markers are poor predictors of risk. The US Guidelines for Use of ARV Agents in Children recommends starting ARV in all symptomatic infants. Data from European cohorts have demonstrated that initiation of treatment prior to the age of six months, leads to significantly better clinical outcomes. [18],[19] However, data from studies showing higher virological failure (and hence, increased risk of development of resistance) among infants started on treatment early, have previously extended some caution in choosing this approach, particularly in asymptomatic infants. [20] Suboptimal virological response in this age group can be attributed to very high baseline viral load levels, poor adherence to complex regimens with poor-tasting drugs and the lack of adequate pharmacokinetic studies to provide drug dosing data for some ARVs. A recent study from South Africa has clearly demonstrated that starting HAART in asymptomatic children with CD4 > 25% before the age of 12 weeks, resulted in 75% reduction in early mortality as compared to a delayed treatment group, which further supports treating all infected infants in the < 12 month age group. [21] In initiating ARV in this age group, consideration should also be given to baseline antiretroviral resistance testing as many infants have been shown to harbor drug-resistant, perinatally transmitted viruses. The following recommendations are based on the guidelines developed by the US Working Group in Antiretroviral Therapy and Medical Management of HIV-Infected Children. [16] The reader is also referred to the WHO/UNAIDS Guidelines for antiretroviral therapy in children. [17] In terms of initiating ARV, experts tend to view the infant younger than 12 months old differently from the older child.
Treatment of children older than 12 months
Risk of disease progression and death in this age group is considered to be lower. Therefore, many experts recommend delaying the initiation of treatment in the subset of children in this age group who are asymptomatic or mildly symptomatic (CDC category A or N) and have CD4+ cells> 25% and viral load < 100,000 copies/mL. Therapy should be strongly considered among those who are asymptomatic (Category A or N) or have mild symptoms, and have CD4+ cells> 25% and have viral load> 100,000 copies/mL. Children who have AIDS or have significant HIV-related symptoms (Category B or C) and those with CD4+ cells < 25% should be treated regardless of symptoms. In children ≥5 years, CD4+ cell numbers may be used in place of CD4+ cell % as age-related CD4+ cell number variability is no longer a concern at this age. In this situation, treatment may be deferred in asymptomatic children who have CD4+ cells> 350 cell/mm 3 and viral load < 100,000 copies/mL. In children who are asymptomatic or mildly symptomatic and have CD4+ counts> 350 cells/mm 3 and have viral load> 100,000 copies/mL, treatment should be strongly considered, but may be deferred, especially if adherence concerns exist. In this age group, all children with AIDS or significant HIV-related symptoms (Category B or C) and those with CD4+ cells < 350 cells/mm 3 should be treated.
Recommended regimen for initial therapy of antiretroviral naive children
The working group on Antiretroviral Therapy published updated guidelines in October 2006. Contrary to the situation in adults, there are few large paediatric trials comparing various HAART regimens, therefore, the recommendations are often based on limited pharmacokinetic data available in children as well as on adult clinical trial data. The following recommendations are based on recommendations made by the working group: [16]
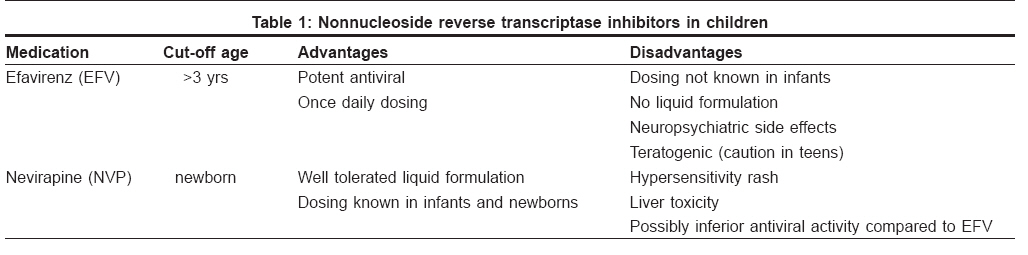
NNRTI-based regimens [Table - 1]
Preferred NNRTI:
- Nevirapine (NVP) + 2 NRTIs for children ≤3 years or those who require liquid formulation
- Efavirenz (EFV)+2 NRTIs for children ≥3 years
Alternative NNRTI:
- Nevirapine+2 NRTIs for children ≥3 years
Efavirenz (EFV) offers the advantage of potent antiviral activity along with ease of once-daily administration, but is not available in a liquid formulation. This limits its use in children ≤3 years who cannot swallow capsules. Furthermore, in sexually active teenage girls, caution needs to be exercised with its use due to the known teratogenic effects of EFV. The neuropsychiatric side effects (fatigue, sleep disturbance, suicidal ideation, and depression) are usually transient, however, EFV should be used with caution in cases of preexisting psychiatric conditions.
Nevirapine (NVP) has been available in a palatable liquid formulation for several years and is well studied in infants and children. Therefore, it offers an attractive option especially for children ≤3 years of age. Hypersensitivity rash and hepatotoxicity are potential toxicities requiring close monitoring.
Delavirdine is not recommended for use in children due to the lack of pediatric data, lower antiviral effect, and higher dosing frequency. Etravirine (TMC 125) has not been studied in children.
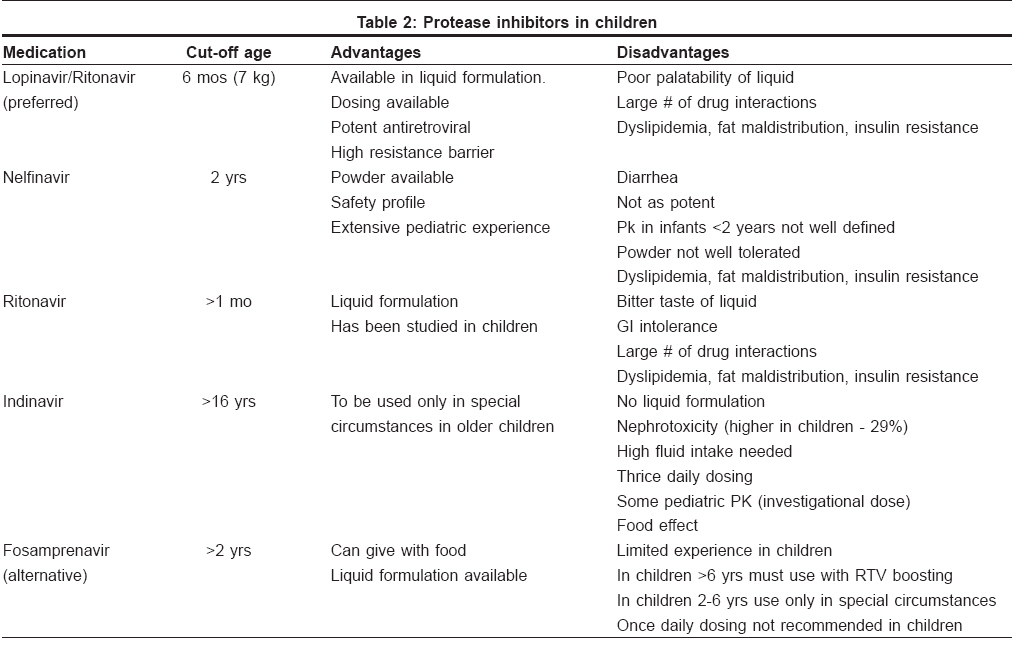
PI-based regimens [Table - 2]
Preferred PI:
- Lopinavir/ritonavir + 2 NRTI
Alternative PI:
- Fosamprenavir + RTV + 2 NRTI (for children ≥6 years)
PIs in general, offer the advantage of potent antiviral effect as well as a high genetic barrier. However, only four PIs have pediatric indications and formulations [Table - 2]. Lopinavir/Ritonavir (LPV/r) is the preferred PI for an initial regimen due to its high potency, high genetic barrier, availability of dosing information even in newborn infants, and low toxicity profile. However, there are no available efficacy data in children comparing LPV/r to other PIs.
Nelfinavir (NLF) was recommended until recently as an alternative PI only in children over two years of age, as dosing information is not available in younger children. Nelfinavir has been shown to have large inter-patient variability in plasma levels, [22] younger children probably require larger doses. [23] Also, in adult trials, NLF has been shown to be inferior to LPV/r in potency. Nelfinavir is available in a powder formulation that is poorly tolerated. Most practitioners recommend crushing the tablets and dissolving in water or other liquid as the preferred way of dosing NLF in children who cannot swallow tablets. However, due to concerns regarding the presence of ethyl methane sulphonate (EMS), a process-related impurity associated with mutagenic carcinogenic potential in animals, the drug is not presently recommended for initiation of ART.
Fosamprenavir (the prodrug of amprenavir) has become available in a liquid formulation since June 2007 and has been approved for use in children> 2 years based on two open label pediatric studies. Full-dose ritonavir or indinavir are not recommended in initial regimens unless there are no other options. A combination of NLF + EFV has been effectively used with two NRTIs in a pediatric study, but is not preferred due to the use of three drug classes at once. [24] In adolescents who are able to be dosed at adult levels, ritonavir-boosted indinavir, fosamprenavir, or saquinavir can be used in initial regimens if no other options are available.
Due to lack of pediatric data, atazanavir, darunavir, tipranavir, and dual PI regimens are not recommended for initial therapy in children. For adolescents, dual PI combinations of fosamprenavir + amprenavir (due to additive toxicity of the same active moiety) and atazanavir + indinavir (increased risk of hyperbilirubinemia) are also not recommended.
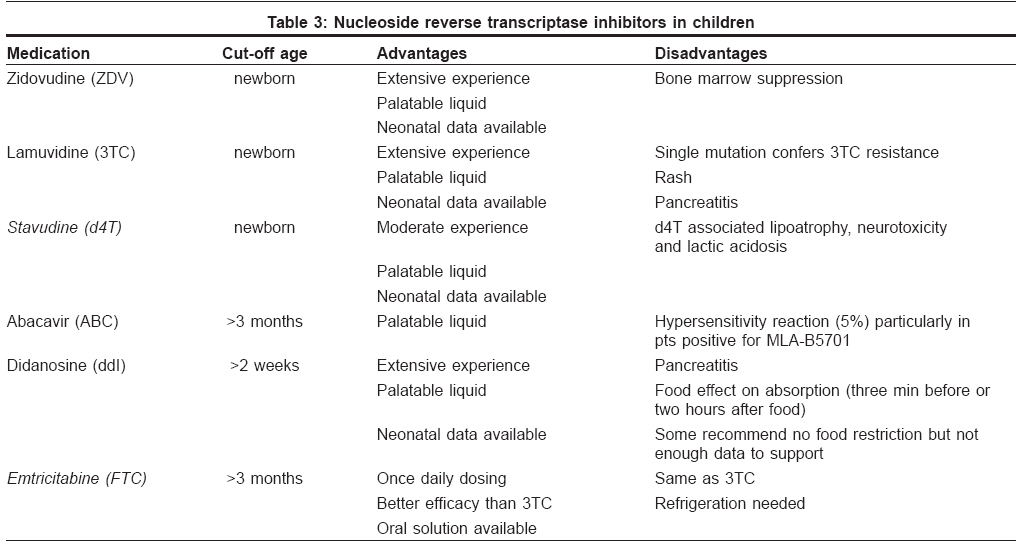
NRTI use in children [Table - 3]
Preferred 2 NRTI backbone
- ZDV + (3TC or ddI or FTC)
- ddI + (3TC or FTC)
Alternative
- ABC + (ZDV or 3TC or FTC or D4T)
- D4T + (3TC or FTC)
A significant level of experience exists with the use of NRTIs in children which forms the essential component of the backbone of HAART regimens; all six currently approved NRTIs have been studied in children. Advantages and disadvantages of the individual agents are listed in [Table - 1]. The majority of pediatric experience has been with ZDV + 3TC, ZDV + ddI, ddI + 3TC. However, less experience exists with FTC as it is similar to 3TC and has little advantage in preferred regimens. Abacavir (ABC)-containing regimens are recommended as alternatives because of its potency despite the potential for a life-threatening hypersensitivity reaction. Stavudine-containing regimens are considered alternatives due to the higher risk of lipoatrophy and lactic acidosis with the use of D4T. The combination of D4T and ddI is recommended only when no other alternative exists as studies in adults have shown increased risk of neurotoxicity, lactic acidosis, and lipodystrophy with this combination. A combination of ZDV and D4T is not recommended due to potential viral antagonism. 3TC and FTC are not recommended as they are essentially similar in structure. Although an investigational powder formulation of Tenofovir is being studied in children, it is not recommended in initial regimens in children < 18 years due to the lack of data, and concerns regarding renal and potential bone toxicity.
Triple NRTI combination
Adult studies have demonstrated the virological inferiority of triple NRTI regimens when compared to EFV-based or PI-based regimens. [25] As few comparative pediatric trials exist, the triple NRTI regimens (ABC + 3TC + ZDV or Trizivir) are recommended as initial regimens based on adult data, only if a PI-based or NNRTI-based regimen cannot be used due to concerns of toxicity or adherence. Other triple drug regimens such as TNF + ABC + 3TC or TNF + ddI + 3TC are not recommended due to adult data demonstrating inferior virological response. [26]
Newer drugs
HIV Fusion inhibitor (Enfuvirtide (T-20)) has been used in a small cohort of previously treated children and has been approved for use in children> 6 years of age based on safety data; [27] there have however, been no large-scale safety trials. Other classes of drugs such as integrase inhibitors (raltegravir) and entry inhibitors (maraviroc) have not been studied in children.
Management of Previously Treated Children
Despite initial success, which can often last for several years in many children, treatment failure often occurs which requires reassessment of treatment options. The reasons for treatment failure, defined as suboptimal response to chosen regimens or virological rebound after initial success, include poor adherence, drug intolerability, drug interactions, inadequate drug levels or poor antiviral activity of the selected regimen. Also, in some cases, virological failure is not associated with immunological or clinical failure. All of these factors must be reassessed before any switch is made to a new antiviral regimen.
Children have fewer antiretroviral agents to choose from, which poses another challenge in achieving the "ideal" undetectable level, especially in patients who have been heavily treatment in the past. In choosing a new regimen, it is important to carefully consider the likelihood of achieving full suppression or adequate antiviral response based on characteristics such as genotypic analysis, availability of at least two tolerable and fully active drugs in the new regimen, and most importantly, the likelihood of adherence over time. Specific recommendations in specific circumstances can be complicated and may require consultation with a specialist knowledgeable in the field of paediatric HIV. Further guidelines for selecting new regimens can be found in the recommendation of the HRSA working group. [16]
Antiretroviral treatment of HIV in children has evolved tremendously since the early 1990s and continues to evolve as new drugs targeting new sites are developed and studied in children. For clinicians caring for children, it is crucial to understand that for the eventual success of treatment, it is critical to manage the "whole" child within the context of his/her own economic, cultural, psychological, and family environment. The clinician must also understand the complexities of the interaction of chronic illness and child development and develop the sensitivity requisite to manage this very complex and evolving disease.
References
| 1. | Gortmaker S, Highes M, Cervia J, Brady M, Johnson GM, Seage GR 3rd, et al. Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med 2001;345:1522-8. Back to cited text no. 1 |
| 2. | Gona P, van Dyke R, Williams PL, Dankner WM, Chernoff MC, Nachman SA, et al. Incidence of opportunistic and other infections in HIV-infected children in HAART era. JAMA 2006;296:292-300. Back to cited text no. 2 |
| 3. | McConnell MS, Byers RH, Frederick T, Peters VB, Dominguez KL, Sukalac T, et al. Trends in antiretroviral therapy use and survival rates for a large cohort of HIV-infected children and adolescents in the United States, 1989-2001. J Acquir Immune Defic Syndr 2005;38:488-94. Back to cited text no. 3 |
| 4. | Shearer WT, Quinn TC, LaRussa P, Lew JF, Mofenson L, Almy S, et al. Viral load and disease progression in infants infected with human immunodeficiency virus type 1: Women and Infants Transmission Study Group. N Engl J Med 1997;336:1337-42. Back to cited text no. 4 |
| 5. | Abrams EJ, Weedon J, Steketee RW, Lambert G, Bamji M, Brown T, et al. Association of human immunodeficiency virus (HIV) load early in life with disease progression among HIV-infected infants: New York City Perinatal HIV Transmission Collaborative Study Group. J Infect Dis 1998;178:101-8. Back to cited text no. 5 |
| 6. | HIV Paediatric Prognostic Markers Collaborative Study Group. Short-term risk of disease progression in HIV-1-infected children receiving no antiretroviral therapy or zidovudine monotherapy: A meta-analysis. Lancet 2003;362:1605-11. Back to cited text no. 6 |
| 7. | European Collaborative Study. Age related standards for T lymphocyte subsets based on uninfected children born to human immunodeficiency virus 1-infected women: The European Collaborative Study. Pediatr Infect Dis J 1992;11:1018-26. Back to cited text no. 7 |
| 8. | Palumbo, PE, Raskino C, Fiscus S, Pahwa S, Fowler MG, Spector SA, et al. Predictive value of quantitative plasma HIV RNA and CD4 lymphocyte count in HIV-infected infants and children. JAMA 1998;279:756-61. Back to cited text no. 8 |
| 9. | Persaud D, Palumbo P, Ziemniak C, Chen J, Ray SC, Hughes M, et al. Early archiving and predominance of nonnucleoside reverse transcriptase inhibitor-resistant HIV-1 among recently infected infants born in the United States. J Infect Dis 2007;195:1402-10. Back to cited text no. 9 |
| 10. | Rogers A. Pharmacokinetics and pharmacodynamics in adolescents. J Adolesc Health 1994;15:605-78. Back to cited text no. 10 |
| 11. | Buchacz K, Rogol AD, Lindsey JC, Wilson CM, Hughes MD, Seage GR 3 rd , et al. Delayed onset of pubertal development in children and adolescents with perinatally acquired HIV infection. J Acquir Immune Defic Syndr 2003;33:56-65. Back to cited text no. 11 |
| 12. | Committee on Pediatric AIDS. Section on International Child Health. Increasing Antiretroviral Drug Access for Children with HIV Infection. Pediatrics 2007;119:838-46. Back to cited text no. 12 |
| 13. | Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med 2000;133:21-30. Back to cited text no. 13 |
| 14. | Van Dyke RB, Lee S, Johnson GM, Wiznia A, Mohan K, Stanley K, et al. Reported adherence as a determinant of response to highly active antiretroviral therapy in children who have human immunodeficiency virus infection. Pediatrics 2002;109:e61. Back to cited text no. 14 |
| 15. | Watson DC, Farley JJ. Efficacy of and adherence to highly active antiretroviral therapy in children infected with human immunodeficiency virus type 1. Pediatr Infect Dis J 1999;18:682-9. Back to cited text no. 15 |
| 16. | Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Developed by the Working Group on Antiretroviral Therapy and Medical Management of HIV-Infected Children. Available from: http://AIDSinfo.nih.gov. [last accessed on 2008 Feb 28]. Back to cited text no. 16 |
| 17. | Antiretroviral therapy for HIV infection in infants and children: Towards Universal Access: WHO guidelines. Available from: http://www/who.int/hiv/pub/guidelines. Back to cited text no. 17 |
| 18. | Faye A, Le Chenadec J, Dollfus C, Thuret I, Douard D, Firtion G, et al. Early versus deferred antiretroviral multidrug therapy in infants infected with HIV type 1. Clin Infect Dis 2004;38:1692-8. Back to cited text no. 18 |
| 19. | Chiappini E, Galli L, Gabiano C, Tovo PA, de Martino M; Italian Register for HIV Infection in Children. Early triple therapy vs mono or dual therapy for children with perinatal HIV infection. JAMA 2006;295:626-8. Back to cited text no. 19 |
| 20. | Hainaut M, Peltier CA, Gerard M, Marissens D, Zissis G, Levy J. Effectiveness of antiretroviral therapy initiated before the age of 2 months in infants vertically infected with human immunodeficiency virus type 1. Eur J Pediatr 2000;159:778-82. Back to cited text no. 20 |
| 21. | Violari A, Colton M, Geibb D, et al. Antiretroviral therapy initiated before 12 weeks of age reduces early mortality in young HIV infected infants: Evidence from children with HIV early antiretroviral therapy (CHER) study. 4 th International AIDS Conference on HIV Pathogenesis, Treatment and Prevention, July 22-25, 2007; Sydney, Australia. Abstract: LBWES 103. Back to cited text no. 21 |
| 22. | Capparelli EV, Sullivan JL, Mofenson L, Smith E, Graham B, Britto P, et al. Pharmacokinetics of nelfinavir in human immunodeficiency virus-infected infants. Pediatr Infect Dis J 2001;20:746-51. Back to cited text no. 22 |
| 23. | Hirt D, Urien S, Jullien V, Firtion G, Rey E, Pons G, et al. Age-related effects on nelfinavir and M8 pharmacokinetics: A population study with 182 children. Antimicrob Agents Chemother 2006;50:910-6. Back to cited text no. 23 |
| 24. | Starr SE, Fletcher CV, Spector SA, Yong FH, Fenton T, Brundage RC, et al. Combination therapy with efavirenz, nelfinavir, and nucleoside reverse-transcriptase inhibitors in children infected with human immunodeficiency virus type 1: Pediatric AIDS Clinical Trials Group 382 Team. N Engl J Med 1999;341:1874-81. Back to cited text no. 24 |
| 25. | Gulick RM, Ribaudo HJ, Shikuma CM, Lustgarten S, Squires KE, Meyer WA 3 rd , et al. Triple-nucleoside regimens versus efavirenz-containing regimens for the initial treatment of HIV-1 infection. N Engl J Med 2004;350:1850-61. Back to cited text no. 25 |
| 26. | Gallant JE, Rodriguez AE, Weinberg WG, Young B, Berger DS, Lim ML, et al. Early virologic nonresponse to tenofovir, abacavir and lamivudine in HIV-infected antiretroviral-naοve subjects. J Infect Dis 2005;192:1921-30. Back to cited text no. 26 |
| 27. | Church JA, Cunningham C, Hughes M, Palumbo P, Mofenson LM, Delora P, et al. Safety and antiretroviral activity of chronic subcutaneous administration of T-20 in human immunodefiency virus 1-infected children. Pediatr Infect Dis J 2002;21:653-9 Back to cited text no. 27 |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08088t2.jpg]
[dv08088t3.jpg]
[dv08088t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}