 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
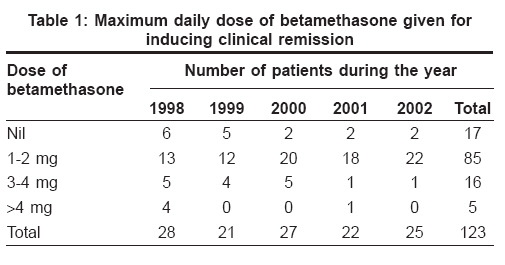
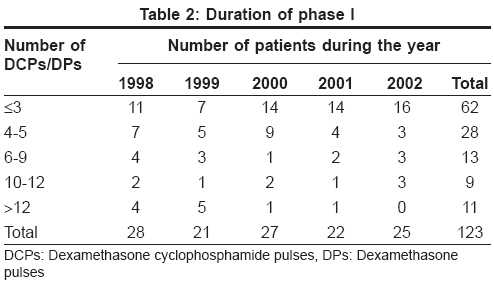
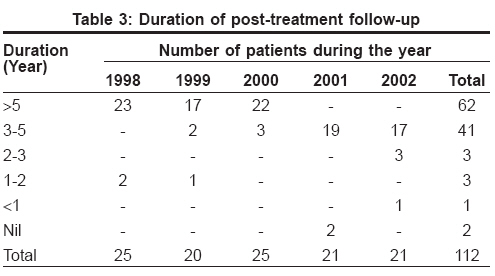
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 217-221 Original Article Current regimen of pulse therapy for pemphigus: Minor modifications, improved results Pasricha JS, Poonam Consultant Dermatologist, Skin Diseases Centre, 1-A, Masjid Moth, DDA Flats, Phase I, Outer Ring Road, Near Chirag Delhi Flyover, New Delhi - 110048 Code Number: dv08090 Abstract Background: If administered properly, dexamethasone cyclophosphamide pulse (DCP) therapy has the potential to effect lifelong recovery from pemphigus. Keywords: Cyclophosphamide, Dexamethasone cyclophosphamide pulse regimen, Dexamethasone, Pemphigus, Pulse therapy Introduction We first used dexamethasone-cyclophosphamide pulse (DCP) therapy for pemphigus in 1982. [1,2] During the subsequent period of 25 years, long-term follow-up of pemphigus patients treated with DCP therapy regimen has revealed that pemphigus can now be considered to be a completely curable disease. [1],[2],[3],[4],[5],[6],[7],[8],[9] Of the first 500 pemphigus patients enrolled by one of us (JSP) for treatment at the All India Institute of Medical Sciences (AIIMS), 57 patients could not/did not continue the treatment for a variety of reasons, and 18 patients died during the treatment. The major reasons for not being able to continue the treatment were long distance from hospital leading to inability to repeatedly report for the treatment and delay in complete recovery in some patients. Most of the deaths were due to unrelated/preventable causes. Of the 425 patients who received the treatment, 236 (55.6%) patients have been in complete clinical remission for more than ten years (many of them for even 20 years) after complete withdrawal of all treatment, and another 77 (18.1%) cases for 5-10 years. This period of confirmed clinical remission has been 2-5 years in 33 (7.8%) patients, 1-2 years in 20 (4.7%) patients, < 1 year, in 25 (5.9%) patients, and no follow-up in 33 (7.8%) cases. Some patients had developed a relapse of pemphigus on stopping the treatment, but these were mostly those who: (1) did not complete the regimen, or (2) were irregular in reporting for the pulses, or (3) were given only one drug (dexamethasone or cyclophosphamide). Repeating the course led to recovery from pemphigus. After JSP′s retirement from the AIIMS, we administered the same regimen in a private clinic with better personal supervision and some modifications. We report here the follow-up of 143 patients enrolled for this regimen over a period of five years (1998 to 2002). Methods Patients Prepulse evaluation included taking a detailed clinical history and performing an examination to look for any concomitant disease or side effects of the previous treatment. The laboratory evaluation consisted of a complete hemogram (hemoglobin, total leukocyte and platelet counts and erythrocyte sedimentation rate), blood sugar, blood urea, serum creatinine, serum glutamate transaminases, serum sodium and potassium, urinalysis, X-ray of the chest, and electrocardiogram. Expert advice was obtained from the concerned specialist if there was any concomitant disease (but homeopathic and Ayurvedic drugs were not allowed). The DCP comprised of 100 mg dexamethasone dissolved in 500 mL of 5% glucose given as an intravenous infusion over approximately two hours, repeated on three consecutive days. On the second day, the patients also received 500 mg of cyclophosphamide added to the dexamethasone infusion. This constituted one DCP. The DCPs were repeated after exactly 28 days from the first day of the drip. Any deviation from the 28-day cycle was considered as irregular treatment. Patients who were unmarried or those who wished to have children in the future were given only dexamethasone and no cyclophosphamide in the pulse (DPs), while diabetic patients received ten units of soluble insulin for each bottle of 500 mL 5% glucose used for the infusion, in addition to their antidiabetic treatment. All patients received 50 mg cyclophosphamide orally, between the pulses every day. In addition, all patients who had active disease were given an adequate daily oral dose of betamethasone to control the disease and to induce quick healing. Those patients who had skin lesions also received systemic antibiotics (usually ciprofloxacin or cefadroxil) in appropriate doses and oral anti-candida drugs if they had oral ulcers. This was supplemented with topical corticosteroids, antibiotics and anti-candida agents. The patients were also encouraged to clean their skin, especially the affected areas with a normal soap for the skin and a shampoo for the hair every day. Oral hygiene was maintained with normal brushing even when the patient had oral ulcers. The use of mild or medicated soaps and shampoos was prohibited. Systemic antibiotics were withdrawn when the skin lesions healed completely, while anti-candida drugs were withdrawn when the mucosal lesions healed fully. After achieving complete clinical remission, the daily oral dose of betamethasone was tapered stepwise and withdrawn completely, while the DCP/DPs, and the daily oral cyclophosphamide were continued. Phase I was the period lasting until the complete tapering of the oral betamethasone and other drugs. During phase II, the patients remained completely normal but DCPs/DPs were repeated in exactly 28-day cycles along with 50 mg daily cyclophosphamide. This phase lasted for nine months. After completing phase II, the DCPs/DPs were stopped while the daily oral dose of 50 mg cyclophosphamide was continued for the next nine months; this was called phase III. Subsequently, all treatment for pemphigus was withdrawn, and the patient was instructed to live like a normal individual - no inhibitions, no prohibitions, and report in case of any problems or once a year for at least ten years (Phase IV). The laboratory evaluations including the immunofluorescence tests were repeated after completing phase II and phase III. Results A total of 143 patients reporting for pemphigus during the five years from 1998 to 2002 were enrolled for the DCP/DP regimen. Of these, 134 had pemphigus vulgaris, five had pemphigus foliaceus and four had pemphigus erythematosus. Seventy eight were males and 65 were females. Three patients were younger than 15 years in age, ten patients were older than 60 years in age, while 73 and 57 patients respectively were in the age groups of 15-40 years and 40-60 years; the overall age range was 7-71 years. Of the 143 patients, 17 patients did not start/continue the treatment, while three patients died during the treatment; these have therefore been excluded from the analysis. The remaining 123 patients received the treatment. The maximum daily dose of betamethasone given to the patients during phase I was nil in 17 patients, 1-2 mg in 85 patients, 3-4 mg in 16 patients and> 4 mg in five patients [Table - 1]. The duration of phase I was ≤3 months in 62 patients, 4-5 months in 28, 6-9 months in 13 patients, 10-12 months in nine patients and> 12 months in 11 patients [Table - 2]. Twenty patients were given DPs and 103 patients received DCPs. Eighty-eight patients who received DCPs and 13 patients who received DPs completed the regimen strictly as per the criteria. On the other hand, nine DCP patients and five DP patients did not complete the regimen, and six and two patients, respectively were irregular in receiving the DCPs/DPs. Eight DCP and three DP patients developed a relapse; the relapse rates therefore, have been 7.7 and 15.0% with DCPs and DPs, respectively. All the 11 relapsed patients were given a second course of the DCP/DP regimen, of which two patients relapsed again but recovered on further treatment. At present, all the patients are in complete clinical remission without any maintenance treatment for pemphigus. Until now, the duration of posttreatment follow-up has been> 5 years in 62 patients, 3-5 years in 41 patients, 2-3 years in three and 1-2 years in three, < 1 year in one with no follow-up in two patients [Table - 3]. The titers of indirect immunofluorescence tests before and after the treatment show a clear shift towards negativity after the treatment [Table - 4]. Discussion These data further confirm that the DCP regimen discussed here can cure pemphigus. If a patient does not get a relapse of the disease without any maintenance treatment for five years, it is reasonable to presume that the patient has been cured. And in cases where the posttreatment follow-up period is> 10 years or even 20 years, there should be no doubt that the disease has indeed been eliminated. This regimen therefore can be considered to cure pemphigus although the optimum result can be obtained only if the regimen is used strictly as per our criteria. Other centres or studies, [10],[11],[12],[13],[14],[15],[16],[17] which do not strictly follow the parameters of our regimen are bound to get different results, and therefore, their results are no reflection on the success of our regimen. Our earlier studies [1],[2],[3],[4],[5],[6],[7],[8] had revealed that the major causes of relapse in the patients treated with the regimen had been, (1) incomplete treatment, (2) irregular treatment, and (3) use of one drug instead of the two mentioned in this paper. The current group of patients followed the instructions more stringently because the need to complete the treatment and to take the DCPs in the fixed 28-day cycles was repeatedly stressed at every visit. Thus, there were only a few patients who stopped reporting to us and some patients still made mistakes in taking the DCPs in the 28-day cycles. The rate of relapse among those who strictly followed the instructions was reasonably low (< 10%). The relapse in these cases was possibly due to the fact that the fixed amount of treatment administered during phases II and III, was presumably not sufficient in these patients to suppress the autoimmune process completely. It is also possible that these patients missed taking the treatment at some stage, but did not tell us the same because of fear of a reprimand, or they happened to take spurious medicines which would also amount to interrupting the treatment. In any case, the second course given to the relapsed cases was able to induce remission all over again. As expected, the relapse rate in the patients given DPs was higher. The three modifications instituted in the current regimen, viz ., (1) emphasis on thorough cleaning of the skin, scalp and oral cavity even when there were lesions, and (2) use of oral antibiotics and anti-candida drugs predictably helped to clear up/prevent the superadded infections which are likely to delay the healing of the lesions, (3) Simultaneous use of oral corticosteroids in doses sufficient to control the disease activity led to quick healing of the lesions and a psychological benefit to the patient. This has been clearly reflected in shortening the duration of phase I to 3-4 months in most of the patients although there were still a few patients who took longer to achieve complete clinical remission. We believe that patients who did not pay adequate attention to cleaning and those who were not given adequate doses of oral corticosteroids and antibiotics took longer to recover completely. It is very important to achieve a complete clinical remission and be able to withdraw oral corticosteroids completely before the patient can be considered to have reached phase II of the regimen. During phase II, the patients should remain completely free of any pemphigus lesions, and complete the mandatory nine DCPs in 28-day cycles. In case the pemphigus lesions recur, the patients should be reverted back to phase I and given more treatment until they achieve complete clinical remission. Phase II should be considered to have been completed only if the patients remain completely free of any pemphigus lesions for a continuous period of nine months. In case of doubt, it is preferable to give a few more DCPs rather than risk a relapse in the future. Completing the nine months of phase III (50 mg cyclophosphamide per day) seems to be equally important. Any attempt to stop the treatment earlier has also been observed to be associated with the relapses in some cases. With the current regimen therefore, it has been possible to reduce the duration of phase I in most of the cases to 3-4 months only. The duration of phases II and III having been fixed at nine months each, the total duration of treatment comes to approximately two years. Out of these two years, the patient suffers from clinical lesions for only the first 2-3 months after which the patient is quite normal and thus, can attend to his/her normal duties/responsibilities. Completing the treatment during phases II and III serves to prevent a relapse in the future. In our experience the side effects of pulse therapy are far less compared to the conventional method of administering corticosteroids and other immunosuppressive drugs. This is further borne out by the findings that the side effects of the current pulse therapy regimen have been observed only during phase I when the patient was receiving additional daily oral corticosteroids. During phase II, the patients regained their normal appearances and could resume their normal professional/social duties. The high incidence of bacterial/candidial infections observed in the earlier studies was not seen in this study. After the skin/oral lesions healed and the other drugs had been withdrawn, the patients were advised not to observe any precautions, and were rather encouraged to live like normal individuals. Muscle weakness (myopathy), diabetes, hypertension, peptic ulceration, osteoporosis etc. do not occur with pulse therapy, although these may manifest when the patient is having additional daily corticosteroids during phase I. These conditions therefore, are not a contra-indication for pulse therapy, but require additional appropriate treatment. The most common side effects during this period consist of: (1) a feeling of weakness and lethargy for 3-4 days after the pulse. This can either be ignored or treated with a tablet of betamethasone daily for 2-3 days after the pulse, (2) Gonadal failure manifesting as amenorrhea/azoospermia which is mostly due to the cyclophosphamide component of the pulse. Use of DPs reduces the risk of gonadal failure but increases the risk of a relapse of pemphigus. By this time, if the patient already has a family, he/she can now be treated with the DCP regimen with appropriate outcomes. The risk of hemorrhagic cystitis, diffuse hyperpigmentation and vascular necrosis is insignificant/nonexistent among our patients, unless they have received these drugs before reporting to us. As the alternative methods of treatment [18],[19],[20],[21],[22] used elsewhere in the world, have never so far been shown to produce equivalent results, pulse therapy should be the first (and the only) choice for treatment in all pemphigus patients until some better regimen evolves. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08090t2.jpg] [dv08090t3.jpg] [dv08090t1.jpg] [dv08090t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}