 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
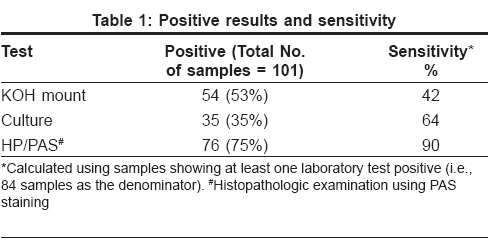
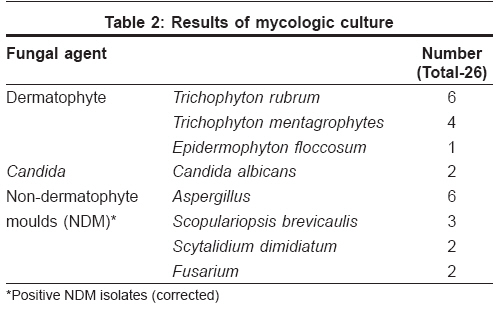
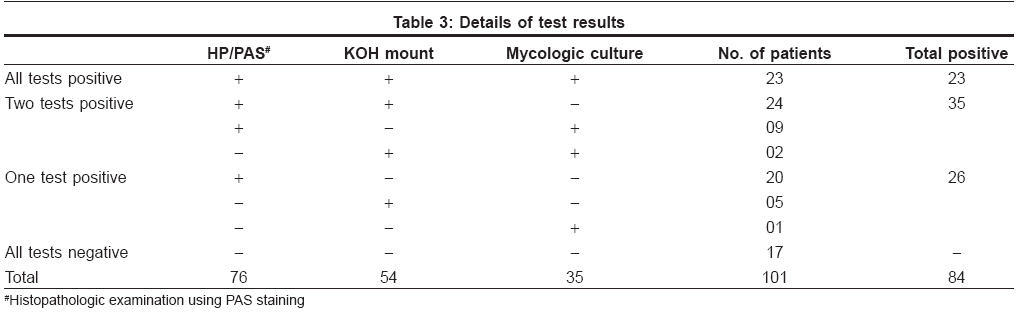
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 226-229 Original Article Comparison of potassium hydroxide mount and mycological culture with histopathologic examination using periodic acid-Schiff staining of the nail clippings in the diagnosis of onychomycosis Shenoy MManjunath, Teerthanath S, Karnaker VimalK, Girisha BS, Krishna Prasad MS, Pinto Jerome Department of Dermatology, K. S. Hegde Medical Academy, Mangalore, Karnataka Code Number: dv08092 Abstract Background: Onychomycosis is a common problem noticed in clinical practice. Currently available standard laboratory methods show inconsistent sensitivity; hence there is a need for newer methods of detection. Keywords: Culture, Onychomycosis, Periodic acid-Schiff staining, Potassium hydroxide mount Introduction Onychomycosis is a common problem in clinical practice, accounting for up to 50% of all nail diseases. [1] It is caused by a variety of fungal agents and presents in several clinical forms. It can mimic several diseases in the field of dermatology and internal medicine. It is necessary to diagnose the infection with some laboratory evidences before treating them with antifungal drugs, whose duration of treatment is long and may have some serious side effects. Currently available routine laboratory methods are direct microscopy with potassium hydroxide mount (KOH) and mycological culture. These traditional methods give inconsistent results, and the results may be altered depending on the method of collection and preparation of specimen. [2] There are many reports in the recent literature on histopathologic diagnosis using periodic acid-Schiff (PAS) staining of nail plates as a useful diagnostic test. [2],[3],[4],[5],[6] This study was carried out to determine the sensitivity of this test in the diagnosis of onychomycosis as compared to that of KOH mount and mycological culture.Methods A total of 101 patients (61 males and 40 females) with clinically suspected onychomycosis under consideration for the treatment were selected for the study. Their ages ranged from 16 to 80 years (mean, 45.2 years). Affected nails were cleaned to remove contaminants and were clipped short with nail clippers. Scrapings were collected from the involved nail bed and from the undersurface of the nail as proximal to the cuticle as possible with a no. 15 scalpel blade. Nail clippings were sent for histopathologic examination with PAS staining, and clippings and scrapings were subjected to potassium hydroxide (KOH) mount and mycological culture. Potassium hydroxide mounts Mycological culture PAS staining Results so obtained were tabulated, and statistical evaluation of the results was done. Results Out of the 101 patients, direct microscopy with KOH mount, mycological culture, and histopathologic examination with PAS staining showed positive results in 54 (53%), 35 (35%), and 76 (75%) patients respectively [Table - 1]. Hence mycological culture was the least sensitive, and HP/PAS was the most sensitive among the tests. Culture yielded growth in 35 (35%) patients, with dermatophytes in 11 (31%), Candida in 2 (6%), and non-dermatophyte moulds (NDM) in 22 (63%) patients [Table - 2]. Similar significantly high non-dermatophyte isolation has been reported earlier. [9],[10] Aspergillus species were the leading NDM isolates (15), and Scopulariopsis (3), Scytalidium (2), and Fusarium (2) were also isolated [Table - 2]. It is difficult to interpret the role of non-dermatophyte mould because the same fungi that can be laboratory contaminants are also occasionally found to be pathogens. [11] Hence it is suggested that if agents other than dermatophytes are isolated, they are probably laboratory contaminants unless KOH or microscopy demonstrates atypical hyphae associated with non-dermatophyte moulds or if the same organism is repeatedly isolated. [11] Using these criteria, only 13 (Aspergillus, 6; Scopulariopsis, 3; Scytalidium, 2; and Fusarium, 2) out of the total 22 non-dermatophyte moulds isolated qualify as true pathogens. In 20 patients, PAS staining was the only evidence of fungal infection [Table - 3]. Therefore, if this test was not done, all these samples would have been falsely reported as negative. Laboratory evidence of fungal infection was obtained in 84 out of the 101 samples by at least one of these three methods being positive. Using this as the denominator, HP/PAS had a sensitivity of 90%, which was significantly higher compared to that of KOH mount (64%) or mycological culture (42%). Statistical analysis of the result was done using McNemar′s test. Comparison of HP/PAS results with those of KOH mount and culture was done, and the variations were statistically significant ( P values < 0.001). It was difficult to comment upon the specificity of these tests since we did not consider any single test as the gold standard. Discussion Onychomycosis is difficult to treat as compared to most other dermatophytoses because of the inherent slow growth of the nail. [11] Older antifungal agents like griseofulvin are unsuitable for onychomycosis because of their relatively poor efficacy and longer duration of treatment. Newer antifungal agents like itraconazole and terbinafin offer higher cure rates. The shortened treatment durations and intermittent (pulsed) dosing schedules have been designed to enhance compliance and reduce the cost of therapy. Because of all these reasons, nowadays a number of patients with onychomycosis receive oral antifungal drugs. These newer drugs also have some potential for serious side effects. It is necessary to confirm the clinical diagnosis with sufficient laboratory evidence before initiating treatments in these patients. Direct demonstration of fungal elements with KOH mount and the isolation of fungus by culture are the routinely done laboratory methods. The method of obtaining nail clippings and the size of specimen are also important factors while considering these tests. Reported sensitivity of fungal culture for identifying dermatophytes varies from 25% to 80% with an approximately 30% false-negative results with culture and KOH studies. [12] These high false-negative results are unacceptable; hence there is need for a test with higher sensitivity that also gives an early diagnosis. DNA-based techniques are currently being used to identify a number of pathogens and may soon be used regularly in the diagnosis of onychomycosis. [13] These tests are likely to be more expensive and may not be available in all centers dealing with nail infections. In the literature, there are reports on histopathologic examination with PAS staining (HP/PAS) of nail clips as a highly reliable diagnostic tool for onychomycosis. [2],[3],[4],[5],[6] Periodic acid-Schiff (PAS) stain demonstrates the presence of certain polysaccharides present in the walls of fungal hyphae. We carried out this study in order to reaffirm whether the probability of pathogen identification by HP/PAS differs significantly from that by KOH mount and mycologic culture. Our results are at par with the results obtained by other authors like Weinberg JM et al. and Lawry et al . [2],[6] Weinberg JM et al. evaluated 105 patients with onychomycosis with four diagnostic tests, namely, KOH preparation, culture, HP/PAS, and calcofluor white stain. They obtained sensitivities of 80% for KOH mount, 59% for culture, and 92% for HP/PAS as compared with calcofluor white staining, which was chosen as the gold standard for statistical purposes. [2] Lawry et al. found HP/PAS to be 85% sensitive. In their study, sensitivities for potassium hydroxide dissolution and centrifugation, combined with PAS, fluorescent brightener, or chlorazol black E, were 57%, 53%, and 53% respectively for the three combinations. [6] Culture on Sabouraud′s agar with chloramphenicol and cycloheximide (Mycosel agar) was 32% sensitive; and on Littman-oxgall agar, it was 23% sensitive. [6] It may hence be concluded that HP/PAS undoubtedly has a higher sensitivity compared to KOH mount or mycological culture. KOH mount is a simple, rapid, inexpensive test to perform, which requires minimum infrastructure but some amount of experience to interpret the smears. [7] Reported false-negative rates are relatively high, but it may score over mycologic culture in its ability to detect fungal agents. [10] Culture is generally considered as the gold standard since it is the only test in routine use that can identify the species of fungus causing onychomycosis. Reported false-negative results are high and may vary based on the experience of the laboratories. [12] False-negative results in culture may arise if the nail sample contains only nonviable organisms, when insufficient sample is collected, when the nail sample is clipped distal to the fungal growth, or if the sample is not crushed before subjecting to the test. [2] A modification of standard method of culture (Trypsin treatment) has also been suggested to improve sensitivity. [14] Identification of fungal elements on microscopy after PAS staining is simple since the spores and mycelia can be seen as conspicuous intensely stained reddish structures. However, precise identification of pathogen and determination of its vitality is not possible. It is more expensive compared to the KOH mount; however, the cost is not high when compared to the total cost of the treatment of onychomycosis. For all the reasons mentioned below, HP/PAS can be considered as an invaluable test in the evaluation of onychomycosis and may also score over the other tests.
Acknowledgment We thank Mrs. Sumathi Prabhu, Lecturer in Biostatistics, A. B. Shetty Memorial Institute of Dental Sciences, Deralakatte, India, for her help. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08092t1.jpg] [dv08092t2.jpg] [dv08092t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}