 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
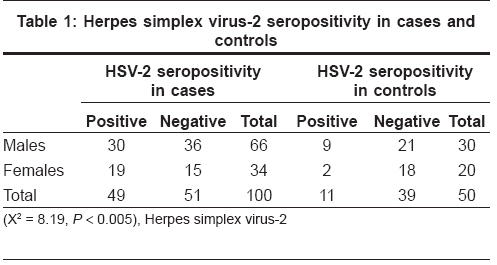
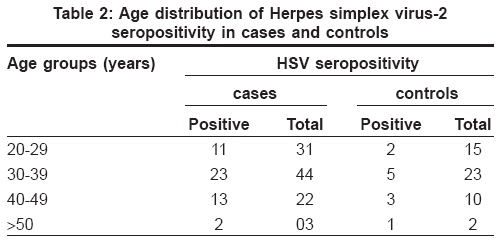
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 230-233 Original Article Herpes simplex virus 2 infection: A risk factor for HIV infection in heterosexuals Anuradha K, Singh HMaan, Gopal KVT, Rama Rao GRaghu, Ramani TV, Padmaja Jyothi Department of Dermatology, Andhra Medical College, Visakhapatnam, Andhra Pradesh Code Number: dv09093 Abstract Background: Genital ulcerative disease is one of the risk factors for acquisition of HIV. As HSV-2 infection is currently the most common cause of genital ulcerative disease, it acts as a potential risk factor for HIV infection. The present study was undertaken to know the seroprevalence of antibodies to HSV-2 in HIV seropositive individuals and in the general population, and to ascertain if HSV-2 is a risk factor for developing HIV infection. Keywords: Human immunodeficiency virus, Herpes simplex virus 2, Seroprevalence Introduction Genital ulcerative disease is one of the risk factors for acquisition of human immunodeficiency virus (HIV) infection because of the disruption of the epithelial barrier and infiltration by CD4+ lymphocytes which are targets for HIV infection. In the recent decades, prevalence of herpes simplex infection is on the rise [1],[2],[3] and herpes simplex virus 2 (HSV-2) infection is currently the most common cause of genital ulcerative disease. [4],[5],[6] Hence, HSV-2 may act as a potential risk factor for the acquisition of HIV infection. [7],[8],[9],[10] Till now, very few studies have been carried out in Asia to compare the seroprevalence of HSV-2 in HIV-positive individuals with that in the general population. [11],[12],[13],[14] The present study was undertaken to know the seroprevalence of HSV-2 in HIV-positive individuals and in the general population, in and around Visakhapatnam, and to ascertain if HSV-2 is a risk factor for HIV infection. Methods This study was conducted in the Department of Dermatology, King George Hospital, Andhra Medical College, Visakhapatnam between June and December, 2004. The study group included one hundred newly detected cases seropositive for HIV infection, both symptomatic and asymptomatic, irrespective of active genital herpes or history of genital herpes. The HIV status of all the patients was established with ELISA test done as per the NACO guidelines. Patients already on antiretroviral therapy (ART) were excluded. Fifty age- and sex- matched healthy volunteers were included as controls. In all cases, a thorough history was taken including demographic data, age of sexual debut, lifetime number of sexual partners, and past history of any sexually transmitted infection (STI). History of genital herpes and number of such attacks were recorded. A thorough clinical examination along with all relevant investigations like complete hemogram, serum biochemistry profile, complete urine examination etc. were carried out. Venereal disease research laboratory (VDRL) test was also done in all patients and controls. CD4 and CD8 estimations and HIV viral load could not be done. Spouses of both cases and controls were not examined or tested. Five ml of blood was collected from all patients and controls, and diagnostic serology was done for HSV-2 using HSV-2-specific glycoprotein IgG2 by indirect immunoassay using ELISA (using EUROIMMUN, enzyme immunoassay kit of herpes simplex type 2 (HSV-2 IgG)). The EUROIMMUN kit ELISA test specifically detects IgG class antibodies directed against HSV-2 glycoproteinG2. Cross-reactivity with antibodies against HSV-1 leading to false positive results does not occur with ELISA. The test done with this kit, as compared to the western blot for HSV-2, is 98% specific and 100% sensitive. Statistical value ′P′ was calculated using the Chi-square test to know the significance of association between HSV-2 and HIV in the case and control groups. Results Out of 100 HIV cases, 66 were males and 34 were females. The age of the cases varied from 20 to 54 years, with a mean age of 32.5 years. Out of 66 males, 60 were married and 6 were unmarried. History of exposure to multiple partners was obtained from all the males. All the females except one were married. One unmarried female was a sex worker. Twenty-two cases (19 males and 3 females) gave a positive history of genital herpes. Out of these 22 cases, 3 males had active genital lesions at the time of the examination. In the control group, there were 30 males and 20 females with a mean age of 31.5 years. Only in 3 cases, positive history of genital herpes was obtained and active disease was not seen in any of these cases. In all the cases and controls, there was no evidence of any other active STI and the serum VDRL test was negative. In the HIV seropositive group, 49 out of the 100 cases (49%) were seropositive for HSV-2 IgG antibodies, of which 30 were males and 19 were females. In the control group, 11 out of 50 controls (22%) were seropositive for HSV-2 IgG antibody and out of these, 9 were males and 2 were females [Table - 1]. The prevalence of HSV-2 seropositivity was higher among HIV-seropositive females, 19 out of 34 cases (52.94%) when compared to males, 30 out of 66 cases (46.96%). The prevalence of seropositivity for HSV-2 increased with increasing age in both HIV-positive cases and controls [Table - 2]. It was 34.37%, 52.27%, 61.90%, and 66.66% in 20-29, 30-39, 40-49, and> 50 years age groups, respectively. The age group of 30-39 had the highest number of HSV-2 seropositives in both the cases and controls. There was a statistically significant association between HSV-2 seropositivity and HIV seropositivity (X 2 = 8.19, P < 0.005). Discussion Genital ulcerative disease is a potential risk factor for acquiring HIV infection. [8],[15] Several studies have revealed that genital herpes is currently the most common genital ulcerative disease. [4],[5],[6] More recently, several groups have reported that serological evidence of herpes simplex virus type 2 infection is associated with increased HIV-1 infection. [16],[17] Asymptomatic shedders can transmit infection and thus are important epidemiologically for 70% of cases. The risk of shedding increases in individuals with recently acquired HSV-2 (within one year) and in individuals with frequent symptomatic recurrences. [3] In our study, out of 50 controls, history of genital herpes was obtained only in 3 cases, though seropositivity was observed in 11 cases. Similarly, in the HIV-seropositive group, out of 100 cases, history of genital herpes was obtained in 22 and active genital lesions were seen in 3 cases, though seropositivity was observed in 49 cases. These observations reveal that serological examination is an accurate tool to know the seroprevalence of HSV-2 in the general population, particularly in asymptomatic carriers. The present study showed that the seroprevalence of HSV-2 in the general population in our area is around 22%. This observation is almost similar to the observations of Flemming et al [5] and Varela et al, [18] who reported the seroprevalence of HSV-2 infection in the general population of the United States and Spain to be 21.9% and 25%, respectively. Some other previous studies have reported a higher seroprevalence of HSV-2. [19],[20] In the present study of 100 HIV-positive cases, only the heterosexual mode of transmission of HSV and HIV was noted. None of the patients gave any history of homosexual exposure. Similar sexual behavior was observed in the control group, highlighting the sexual behavior pattern of the population in this region. This establishes that heterosexual mode is the main route of transmission of HSV/HIV in this area. The observation of 49% seropositivity for HSV-2 in HIV-positive individuals is in correlation with previous studies. [21],[22] A very high HSV-2 seropositivity in HIV-infected individuals was observed in North America and Africa. [10],[23] It was also observed in the present study that the seropositivity for HSV-2 in HIV cases is slightly higher in females (52.94%) than in males (46.96%). This shows that women are more vulnerable for acquisition of HSV and HIV than men. The present study also showed that the percentage of seropositivity for HSV-2 increased with increasing age of the individuals tested. The age group of 30-39 had the highest number of HIV and HSV-2 seropositives and also the highest number of HSV-2 seropositives among controls. Similar observations were made in earlier studies. [5],[18] These findings reveal that this is the most vulnerable age-group for acquiring these two diseases. Statistical analysis showed that there is a statistically significant association between HSV-2 and HIV infection (X 2 = 8.19, P < 0.005), which is in accordance with previous studies. [10],[22],[23],[24] This once again establishes the role of HSV-2 in acquiring HIV infection. The high seroprevalence of HSV-2 may act as one of the contributing factors for HIV acquisition among heterosexuals. Unlike patients with other genital ulcerative diseases, those who have had genital herpes are often unaware of prior infection, making serological evidence a more accurate predictor of prior genital herpes. These asymptomatic seropositive patients, who continue to engage in unprotected sexual activities, may be responsible for increased transmission of both HSV-2 and HIV to uninfected partners. Genital herpes infections are the commonest cause of disruption of epithelial barrier and infiltration of CD4 cells locally in the genital mucosa. Thus, these infections act as a major risk factor for acquisition of HIV. Early detection, treatment, counseling, and health education of genital herpes cases would play an important role in controlling the dreaded epidemic of HIV. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08093t2.jpg] [dv08093t1.jpg] |
| |||||||||

{kind=link}
{kind=link}