 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
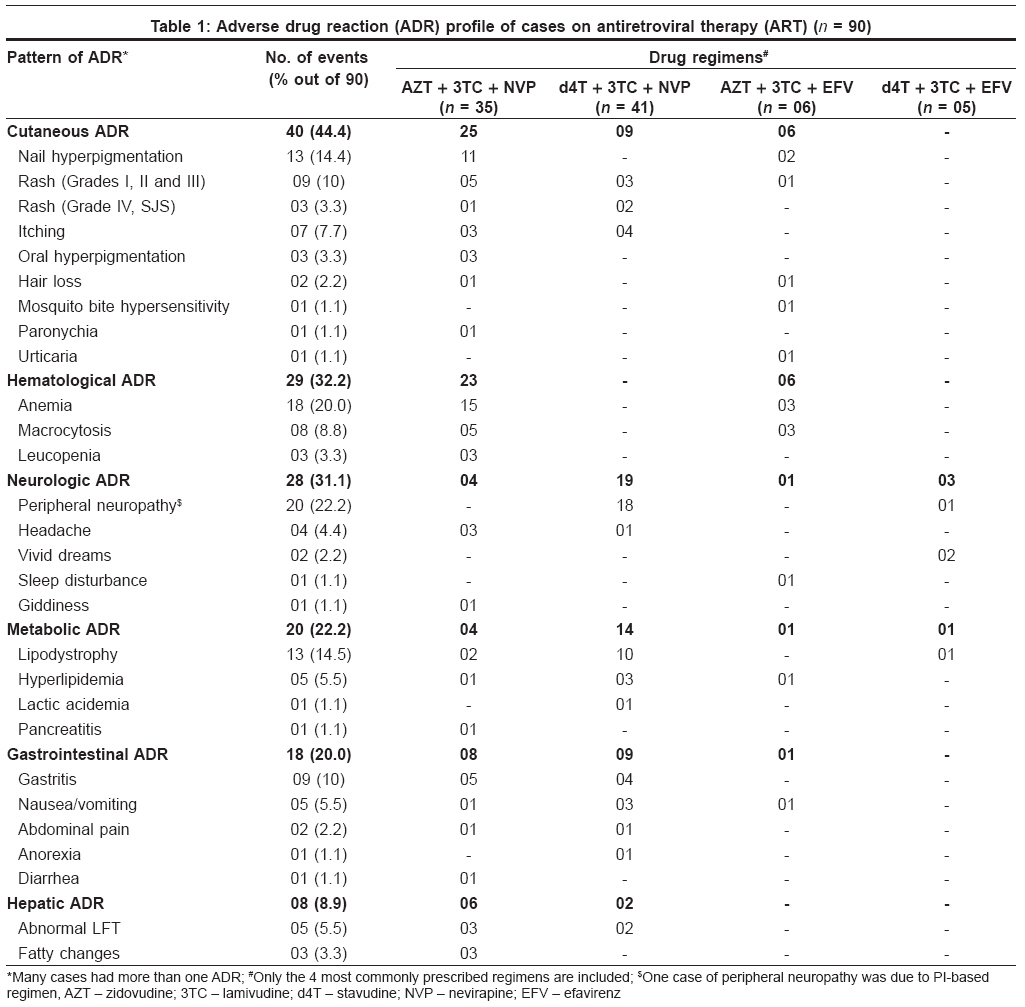
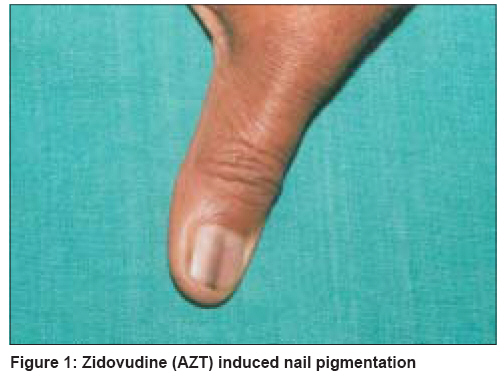
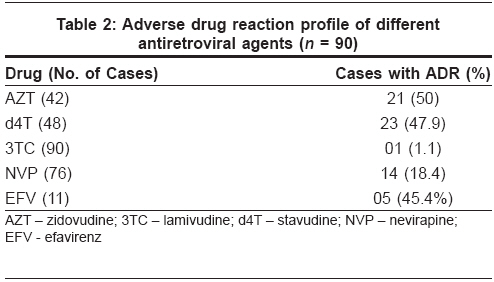
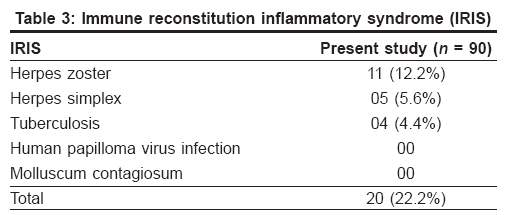
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 234-237 Brief Report Adverse effects of antiretroviral treatment Sharma Ajay, Vora Roshni, Modi Megha, Sharma Archana, Marfatia Yogesh Department of Skin and VD, Medical College and SSG Hospital, Vadodara Code Number: dv08094 Abstract Background: The introduction of highly active antiretroviral therapy (HAART) has led to significant reduction in acquired immune deficiency syndrome (AIDS)-related morbidity and mortality. Adverse drug reactions (ADRs) to antiretroviral treatment (ART) are however, major obstacles in its success. Keywords: Adverse drug reaction, Antiretroviral therapy, Acquired immune deficiency syndrome, Human immune deficiency virus Introduction The introduction of highly active antiretroviral therapy (HAART) has led to a significant reduction in acquired immune deficiency syndrome (AIDS)-related morbidity and mortality. Unfortunately, up to 25% of all patients discontinue their initial HAART regimen because of treatment failure, toxic effects or noncompliance within the first eight months of therapy. [1],[2] Several strategies have been implemented to improve treatment duration. Due to the ongoing development of new antiretroviral agents, prompt understanding and management of adverse effects becomes very important. The sustained benefits of HAART have led to far greater numbers of HIV-1 infected cases receiving at least three drugs for greater periods of time. Moreover, drug-related toxicity is being increasingly recognized because of the declining incidence of HIV1-associated opportunistic infection. The risk of specific side effects varies from drug to drug, from drug class to drug class, and from patient to patient. This paper presents results from our study of adverse drug reactions to antiretroviral therapy (ART) in a cohort of 100 patients from Vadodara, India in a resource-restricted setting. Methods This study was carried out in the HIV referral clinic of the Department of Skin and V.D. from September 2004 to October 2006. In this two-year period, all HIV-positive cases who were already on ART and who were newly started on ART were included and were followed prospectively for the development of any ADRs. One hundred HIV-positive cases who were on ART, were included in this study. A detailed history of every patient was taken including past history of ART. History of fever, cough, breathlessness, past or present history of pulmonary/extrapulmonary tuberculosis (TB), skin lesions, mucosal lesions and sexually transmitted diseases (STD) was taken for every patient. Baseline laboratory investigations such as hemoglobin (Hb), total counts, differential counts, erythrocyte sedimentation rate, urine analysis, serum venereal disease research laboratory (VDRL) test, serum hepatitis B surface antigen (HBsAg), Mantoux test (MT) and fine needle aspiration cytology (FNAC) of lymph nodes were carried out in each patient to rule out any opportunistic infection or specific contraindication to any drug. X-ray of the chest and ultrasonography of the abdomen were done in all cases to determine the focus of TB. Lymphocyte enumeration was carried out before starting antituberculous treatment (ART). Viral load was not advised routinely and patients were also subjected to liver function tests (LFTs), renal function tests (RFTs), lipid profile and blood sugar tests. The three-drug regimen was given to patients who could afford to undergo this treatment. Efavirenz-based regimen was given to patients having TB. All cases on ART were periodically subjected to clinical and laboratory monitoring. They were also screened for opportunistic infections (OIs) and drug toxicity in each follow-up visit during this two-year period. Response to ART was indicated by decreased frequency of infections (bacterial infections, oral thrush and other OIs). CD4 count was done every six months or more frequently if clinically indicated. In patients who were on zidovudine (AZT)-containing regimens, hemoglobin was measured before initiation and at 4, 8 and 12 weeks of therapy or in response to their symptoms. LFTs were done at 2, 4, 8 and 12 weeks in patients on nevirapine (NVP)-based regimens. Lipid profile and serum lactate, serum amylase were done whenever indicated. Plasma viral load was not done routinely but was carried out in case of treatment failure. Assessment of adherence to study medication was based on the patient′s self-report and pharmacy records. Patients were asked to bring empty bottles and strips. Results One hundred cases were enrolled in the study - ten cases were lost to follow-up after the first visit and they were omitted from the study so that 90 cases were available for evaluation. In the present study, ADRs were observed in 64 cases (71.1%) and many cases had ≥ 1 ADR. The most common ADRs were cutaneous (44.4%) [Table - 1]: nail hyperpigmentation (14.4%) and rash (13.3%) [Table - 1]. Rash was mainly observed with Nevirapine-based regimen and in one case with efavirenz (EFV)-based regimen [Table - 1]. The rash was graded according to the AIDS Clinical Trial Group′s grading severity of cutaneous eruptions. [3] Nail and oral hyperpigmentation was attributed to AZT [Table - 1], [Figure - 1]. Anemia was observed after ART containing AZT in 18 cases (20%) [Table - 1] and severe anemia (grade IV, Hb < 6.5 g/dL) was observed in 7.2% of the cases. The most common neurological ADR peripheral neuropathy (PN) (22.2%) was induced by stavudine (d4T) in 19 cases [Table - 1] and by boosted lopinavir (LPV/r) in one case. Lipodystrophy observed in 14.5% of all cases [Table - 1] was due to d4T or AZT. Pancreatitis was observed in a 12 year-old male on AZT + 3TC (lamivudine) + NVP, which could be attributed to 3TC. Gastrointestinal ADRs were seen in 18 cases (20%). Abnormal liver function tests (LFT) were observed in five cases (5.5%) and fatty changes were detected in the liver on ultrasonography in three cases (3.3%) on follow-up. In the present study, fatty changes were observed in AZT-based regimens. Liver mitochondrial toxicity is associated with increased lipid deposits, resulting in micro- or macrovesicular steatosis. The number of cases having ADR with a specific drug was highest with AZT (50%), followed by d4T (47.9%) [Table - 2]. However, the more serious long-term metabolic ADRs were more commonly observed with d4T [Table - 1]. Immune reconstitution inflammatory syndrome (IRIS) was observed as a paradoxical reaction to ART in 20 (22.2%) cases [Table - 3]; TB IRIS was observed in four cases. Two had abdominal tuberculosis detectable on ultrasonography and two had tuberculous lymphadenitis. Seventeen (19%) out of 90 cases were nonadherent to medications and ADRs were the most common reason for irregular treatment in five (29.4%) cases. Discussion Ninety cases were observed over a period of two years; ADRs were observed in 64 of them (71.1%). A Swiss cohort reported ADRs in 74% of their cases. [4] The most common ADRs were cutaneous (44.4%), rash was mainly due to NVP. In all cases with rash, NVP was omitted and the rash was managed conservatively. Later on, EFV replaced nevirapine in the regimen. Other common ADRs in this study were PN (22.2%) and anemia (20%). In a study by Kumarasamy et al. , the most common ADRs were PN, anemia and nail hyperpigmentation. [5] Anemia was seen in 20% of the cases; grade IV anemia was seen in 7.4% cases as compared to 34% in an old study by Van Leeuwen et al. [6] In cases with grade IV anemia (Hb < 6.5 g/dl), AZT was replaced by d4T and the remaining cases were managed conservatively with iron and folic acid supplementation. Peripheral neuropathy was mainly seen with d4T and d4T was replaced by AZT in all cases. Lipodystrophy was observed in 14.5% of the cases while Thierry Saint Marc et al. reported it in 46.5% of their cases. [7] Lactic acidemia, a subtle manifestation of lactic acidosis, was observed in one female. It was diagnosed promptly due to clinical suspicion and proper investigation of serum lactate levels, because of which she was managed effectively. The most common gastrointestinal ADR was gastritis (10%) in the present study. In a study by O′Brien et al. , GI events were mentioned as the most common reason (4.4%) for a patient to discontinue ART due to ADRs. [8] Maniar et al. reported abdominal pain and diarrhea in 0.7 and 0.2% of their cases, respectively, while they were observed in 2.2 and 1.1% of our cases, respectively. [9] Fatty changes observed in the liver on routine ultrasonography were mainly due to AZT-induced mitochondrial toxicity. IRIS was observed in 22.2 and 21% of the cases in our and the King′s College study, respectively. [7] The most common among these was herpes zoster due to IRIS. All cases were managed conservatively and ART was continued. ART is becoming increasingly effective, but also increasingly complex. Adverse effects of therapy may cause symptoms that affect a variety of organ systems. Although current antiretroviral regimens are potent from an antiviral perspective, they often fail because of patient nonadherence. To optimize adherence and hence efficacy, clinicians must focus on preventing adverse effects whenever possible, and distinguishing those that are self-limited from those that are potentially serious. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08094t2.jpg] [dv08094f1.jpg] [dv08094t1.jpg] [dv08094t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}