 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
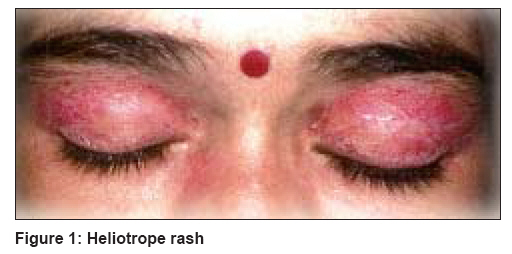
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 241-243 Case Report Dermatomyositis in a human immunodeficiency virus infected person Marfatia YogeshS, Ghiya RaginiA, Chaudhary Dipak Department of Skin and VD, Government Medical College and SSG Hospital, Vadodara Code Number: dv08096 Abstract It is interesting to study an autoimmune condition like dermatomyositis (DM) in the setting of immunosupression due to human immunodeficiency virus (HIV) infection. An HIV seropositive female aged 30 years, presented with a nonitchy rash over the face, breathlessness, diarrhoea and difficulty in raising her hands above her head. A heliotrope rash around the eyes, Gottron's papules and proximal muscle weakness were found to be present. C reactive protein, erythrocyte sedimentation rate and lactate dehydrogenase levels were raised, but creatinine phosphokinase and anti-nuclear antibody profile were normal. Her HIV serostatus was confirmed by Western blotting, keeping in mind the potential for false positive HIV serology in an autoimmune disorder. Her CD4 count was 379 cells/mm 3 . An X-ray of the chest showed bilateral pleural effusion with raised pleural fluid adenosine deaminase levels. Clinical findings and laboratory investigations favored the diagnosis of DM and HIV infection with tuberculous effusion in an HIV seropositive patient. She was treated with antibiotics, four-drug anti-tubercular treatment, systemic steroids and later, antiretroviral treatment. Chances of a false positive antibody test for HIV should be considered in a patient having an autoimmune disease such as DM. Keywords: Dermatomyositis, Human immunodeficiency virus, Tuberculosis Introduction Dermatomyositis is an autoimmune disorder that includes an inflammatory myopathy and characteristic skin manifestations. The etiology of dermatomyositis remains unknown; some studies have reported an association with histocompatibility antigens, environmental agents ( e.g ., virus, drugs) and autoimmunity. [1] It is interesting to study an autoimmune condition such as dermatomyositis in a case having immunosupression due to HIV/AIDS. HIV induces muscle fibres to express the Major Histocompatibility Complex 1(MHC-1), triggering cell-mediated muscle fibre injury. [2] HIV-associated myopathy is common (up to 25%) and can be the result of HIV wasting syndrome, antiretroviral drugs ( e.g ., zidovudine), [3] autoimmune conditions like dermatomyositis, opportunistic infections, endocrinological or metabolic abnormalities and neoplasms. Autoimmune conditions such as dermatomyositis can be responsible for false positive enzyme-linked immunosorbent assay (ELISA) for HIV, but HIV infection can also alter the clinical presentation and course of the autoimmune disease. Moreover, with increasing use of antiretroviral therapy, incidence of autoimmune diseases may increase in HIV-infected patients. [4] Case History A 30 year-old, HIV seropositive female presented with a nonitchy rash over her face along with joint pains, difficulty in raising her hands above her head and climbing stairs since the last six months. She also had complaints of fever, breathlessness, diarrhoea and difficulty in deglutition since one month. Physical examination revealed heliotrope rash around the eyes [Figure - 1], Gottron′s papules on the dorsa of the hands, nail-fold telangiectasias and hypertrichosis over the upper lip with grade III power of the proximal muscles of the thighs and arms. The patient had raised erythrocyte sedimentation rate (60 mm at the end of the 1 st hour), lactate dehydrogenase (LDH, 471 IU/L) levels and tested positive for C-reactive protein (CRP). However, her creatinine phosphokinase (CPK) and alanine transaminase levels were not raised, rheumatoid factor was absent and antinuclear antibody profile was normal. Electromyography showed a myopathic pattern of motor unit action potential with increased insertional and spontaneous activity suggestive of dermatomyositis. Muscle biopsy was not carried out. These clinical features and laboratory findings were suggestive of dermatomyositis. Her HIV serostatus was confirmed by Western blotting, keeping in mind the potential for false positive HIV serology in autoimmune disorders. Her CD4 count was 379 cells/mm 3 . Plasma viral load was not carried out due to cost constraints. A chest X-ray showed bilateral pleural effusion obscuring the underlying lung. Approximately one litre of pleural fluid was tapped. Pleural fluid analysis showed raised total counts with lymphocytic predominance (80%) and increased protein (270 mg/dl). Adenosine deaminase (ADA) level was also elevated in the pleural fluid (152 IU/L), suggestive of tuberculosis (TB). Gram and acid fast bacillus (AFB) stains of smears were negative. Bacterial and AFB cultures showed no growth at the end of six weeks of incubation in LJ (Lowenstein Johnson) medium. Her Mantoux test was found to be nonreactive with 5 TU (tuberculin unit). Left mid-zone consolidation was evident on a chest X-ray after tapping the pleural fluid. Ultrasonography (USG) and computed tomographic (CT) scan of the chest supported the chest X-ray′s findings with no evidence of mediastinal lymphadenopathy. USG of the abdomen did not show any evidence of retroperitoneal lymph nodes or splenic microabscesses. In view of these findings, a diagnosis of dermatomyositis with pulmonary tuberculosis and underlying HIV infection was made. The patient was treated with systemic corticosteroids (oral prednisolone 1 mg/kg/day) in tapering doses and antibiotics (amoxicillin-clavulanic acid 1.2 g intravenously twice a day) along with physiotherapy and photoprotection. She was given oral fluconazole 100 mg once a day for 14 days to treat any possible esophageal candidiasis. However, difficulty in deglutition persisted even after that, suggesting the involvement of oesophageal muscles by myopathic process. Her myopathy improved on follow-up with the power in proximal limb muscles being grade 4+ and a subsidence in difficulty in deglutition. She was put on four-drug anti-tubercular therapy (ATT), i.e ., isoniazid, rifampicin, pyrazinamide and ethambutol for two months followed by two drugs, i.e ., isoniazid and rifampicin for four months. She showed remarkable improvement clinically and radiologically. While on ATT, she developed multiple swellings in the axillae, inguinal regions, legs, forearms and the retromammary region. Fine needle aspiration cytology (FNAC) of these swellings showed clusters of epitheloid cells with little caseous necrosis suggestive of tuberculous lymphadenitis in a case with HIV-induced immunosupression. Smear for AFB was positive on ZN (Zeil Nelson) staining. She was subsequently put on ATT category II, i.e ., isoniazid, rifampicin, pyrazinamide, ethambutol and streptomycin. Although it was not feasible to prove, this could be a case of multidrug resistant (MDR) TB. After one year, her LDH was 637 U/L and CPK was not elevated. Her CD4 count was 251 cells/mm 3 . Later on, she was put on ART comprising of zidovudine, lamivudine and efavirenz due to interaction between nevirapine and rifampicin. Discussion Association of dermatomyositis with HIV infection is rare. Study of such an association of an autoimmune disease with an immunosuppressed state such as HIV infection, brings several interesting and complex issues to the fore. Chances of a false positive antibody test for HIV should be considered in a patient having an autoimmune disease such as dermatomyositis. Difficulty in deglutition in this patient could be due to either oesophageal candidiasis or to oesophageal muscle involvement in dermatomyositis. While investigating such patients, it should be kept in mind that pleural effusion can occur as a part of dermatomyositis or can be due to tuberculosis in the setting of HIV-induced immunosupression. Hence, biochemical and microbiological analyses of pleural fluid are necessary in these patients. Moreover, although CPK levels can be elevated in dermatomyositis, they can be normal when associated with an HIV infection. [5] Roedling et al. reported a case of HIV with polymyositis and normal CPK levels that had been diagnosed on the basis of biopsy. [6] Patients with DM and normal CPK levels may have poorer prognosis with respect to pulmonary disease and associated malignancy. [7] Dermatomyositis in an HIV seropositive case needs to be differentiated from HIV-induced myopathy characterized by elevated muscle enzymes and antiretroviral drug induced myopathy. Myopathies associated with HIV can be due to dermatomyositis/polymyositis, nemalin rod myopathy, zidovudine-induced, rhabdomyolysis, HIV wasting syndrome and myopathies due to local neoplasm or local infection. It is important to distinguish between HIV-induced myopathy, dermatomyositis and steroid-induced myopathy as all three cause proximal muscle weakness. CPK levels are usually high in dermatomyositis, HIV-induced and AZT-induced myopathy, but can be normal when associated with HIV, dermatomyositis and steroid-induced myopathy. [2],[8] Steroid-induced myopathy also shows increased urinary creatinine levels. On EMG, dermatomyositis and HIV-induced myopathy show increased insertional and spontaneous activity, while steroid-induced myopathy shows normal insertional and little abnormal spontaneous activity. Muscle biopsy shows perifascicular atrophy with perivascular T lymphocytes in dermatomyositis, mononuclear infiltrate in HIV and atrophy of type II fibres with no inflammation in steroid-induced myopathy. [7],[9] Moreover, it is important to be aware of steroid myopathy, which may mimic a worsening dermatomyositis. It can be differentiated by neck flexor strength evaluation, which will be unchanged if there is any steroid myopathy. [7],[9] Long-term systemic corticosteroids are first line therapeutic agents for dermatomyositis and need to be used with caution when there is HIV-induced immunosupression. Moreover, antimetabolites such as methotrexate and other immunosuppressives can not be used for treating dermatomyositis in these patients. Tuberculosis along with HIV and steroid-induced immunosupression frequently leads to treatment failure and MDR TB. While considering ART for these HIV-TB co-infected patients, efavirenz is the preferred NNRTI (nonnucleoside reverse transcriptase inhibitor) in the ART regimen as rifampicin is known to lower the serum drug levels of nevirapine. Antiretroviral treatment is indicated in all symptomatic cases with an AIDS-defining illness (extrapulmonary tuberculosis in our case) having CD4 count < 350 cells/mm 3 . [10] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08096f1.jpg] |
| |||||||||

{kind=link}