 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
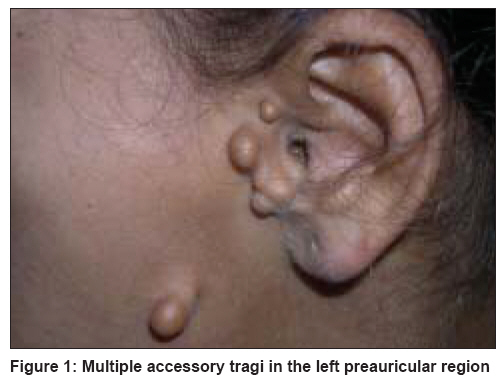
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 254-256 Case Report Goldenhar syndrome with unusual features Mehta Bijal, Nayak Chitra, Savant Shankar, Amladi Sangeeta Department of Dermatology, T.N. Medical College and B.Y.L. Nair Ch. Hospital, Mumbai Central, Mumbai - 400 008 Code Number: dv08100 Abstract We report here the case of a 17 year-old girl with the classic signs of Goldenhar syndrome in the form of multiple accessory tragi, bilateral ocular dermoids, mandibular hypoplasia (micrognathia) and cervical lordosis. She also had a high arched palate, gingival hypertrophy and malaligned teeth, features which are as yet unreported. Keywords: Accessory tragi, Goldenhar syndrome, Oculo auriculo vertebral dysplasia Introduction Goldenhar syndrome (oculoauriculovertebral dysplasia with hemifacial microsomia) is a rare congenital anomaly involving the first and second branchial arches. [1] It is also known as the oculoauriculovertebral syndrome (OAVS) because of the association of eye anomalies with or without vertebral and ear anomalies. [2] Case History A 17 year-old female, born of nonconsanguineous marriage, presented with complaints of congenital, asymptomatic lesions on the face, neck and eyes. There was no increase in the size of the lesions. There was no history of any scholastic backwardness, convulsions or deafness. The child was born of a full-term normal delivery and there was no history of any maternal illness during the pregnancy. All other family members including the two younger siblings were normal. She had attained menarche at the age of 14 years and had no history of any menstrual abnormalities. On cutaneous examination, the patient was found to have a thin narrow face with mandibular hypoplasia. There were multiple, bilateral skin-colored papules in the preauricular area along the line joining the tragus and the angle of the mouth [Figure - 1]. They were also seen above the sternoclavicular joints at the base of the neck [Figure - 2] and were identified as accessory tragi. Examination of the oral cavity revealed a high arched palate, gingival hypertrophy and malaligned teeth [Figure - 3]. Ocular examination showed the presence of bilateral, soft, pinkish-brown nodules on the bulbar conjunctiva and the limbus, identified as dermoids [Figure - 4]. There was also a yellowish, soft lipodermoid on the temporal aspect of the left eye. There was no evidence of any coloboma or micropthalmia. Skeletal examination was clinically normal. Examination of the cardiovascular, respiratory, gastrointestinal and genitourinary systems revealed no abnormality. The patient′s mental and physical development was normal for her age. The patient′s hemogram and blood biochemistry were normal, however, X-ray of the cervical spine revealed lordosis. Other radiological investigations in the form of X-rays of the chest and of the lumbosacral spine and ultrasonography of the abdomen and pelvis revealed no abnormality. Pure tone audiometry revealed no evidence of deafness. ECG and 2D-echocardiography of the heart were normal. We diagnosed the patient as a case of Goldenhar syndrome on the basis of multiple accessory tragi, ocular dermoids, micrognathia and cervical lordosis. She was counseled regarding the condition and underwent surgery for excision of limbal dermoids. Discussion Facioauriculovertebral syndrome was first recorded by the German physician, Carl Ferdinand Von Arlt, in 1845. [3] In 1952, Goldenhar described a patient with a triad of accessory tragi, mandibular hypoplasia and ocular (epibulbar) dermoids and called this constellation of features Goldenhar syndrome. [3] Gorlin et al. named this syndrome oculoauriculovertebral dysplasia due to the presence of additional vertebral anomalies. [4] The incidence of Goldenhar syndrome has been reported to be between 1:3500 to 1:5600, with a male:female ratio of 3:2. [2] The incidence is higher, about 1:1000, in children with congenital deafness. [3] The exact etiology is not known. However, it is possible that abnormal embryonic vascular supply, disrupted mesodermal migration or some other factor leads to defective formation of the branchial and vertebral systems. [2],[5] Most of the cases have been sporadic. Autosomal dominant, autosomal recessive and multifactorial modes of inheritance have also been suggested. [2] Chromosomal studies have not revealed any abnormality. [6] Ingestion of drugs such as thalidomide, retinoic acid, tamoxifen and cocaine by the pregnant mother may be related to the development of this syndrome. Maternal diabetes, rubella and influenza have also been suggested as etiologic factors. [7],[8] In our case, there was no history of maternal drug intake, any febrile illness or diabetes during pregnancy. The classic features of this syndrome include ocular changes such as microphthalmia, epibulbar dermoids, lipodermoids and coloboma; aural features such as preauricular tragi, hearing loss and microtia; and vertebral anomalies such as scoliosis, hemivertebrae and cervical fusion. [1],[2],[5] The abnormalities are found to be unilateral in 85% of cases and bilateral in 10-33% cases. [7] In Goldenhar syndrome, ocular anomalies especially bilateral dermoids are seen in 60% of the cases, vertebral anomalies in 40% of the cases and ear anomalies also in 40% of the cases. [2] Other systemic features are found in about 50% of the patients. [5] Tetralogy of Fallot and ventricular septal defects are the most common cardiovascular anomalies associated with OAVS. [4] Cleft lip and palate, macrostomia, micrognathia, webbing of the neck, short neck, tracheoesophageal fistula, abnormalities of sternocleidomastoid muscle, umbilical hernia, inguinal hernia, urologic anomalies, hypoplastic vagina and anal anomalies may be associated. [1],[5],[7] Anophthalmos, facial palsy, calcification of falx cerebri, undescended testes, and association of Goldenhar syndrome with Turner′s syndrome and glaucoma are the rarer reported associations. [6],[9] Our patient additionally showed a high arched palate, gingival hypertrophy and malaligned teeth, features which are as yet unreported in literature. Other syndromes associated with multiple preauricular tragi include Treacher-Collins syndrome, Wolf-Hirschhorn syndrome, Nager′s acrofacial dysostosis, Wildervanck syndrome (cervicooculoacoustic syndrome), Townes-Brocks syndrome and Delleman syndrome. [5],[10] Treacher Collins syndrome is associated with maxillary and mandibular hypoplasia but is not associated with ocular and aural anomalies. [2] The treatment of the disease varies with age and systemic associations and is mainly cosmetic in uncomplicated cases. In patients with mandibular hypoplasia, reconstruction can be done with rib grafts and an underdeveloped maxilla can be lengthened by a bone distraction device. Reconstruction surgeries of the external ear may be performed at the age of 6 to 8 years. In patients with milder involvement, jaw reconstruction surgeries can be done in the early teens; epibulbar dermoids should be surgically excised. [2],[7] Structural anomalies of the eyes and ears can be corrected by plastic surgery. [2] Prognosis of the disease is good in otherwise uncomplicated cases without any systemic associations. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08100f3.jpg] [dv08100f1.jpg] [dv08100f4.jpg] [dv08100f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}