 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
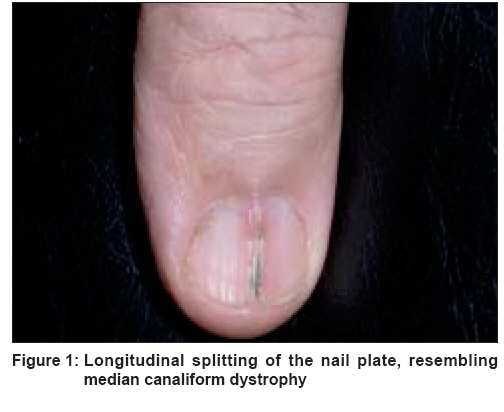
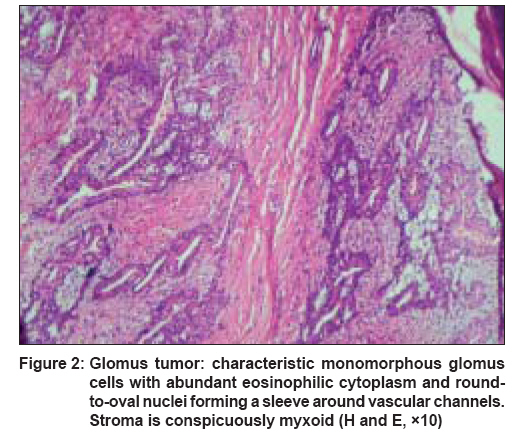
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 257-259 Case Report Glomus tumor-induced longitudinal splitting of nail mimicking median canaliform dystrophy Verma SB Consultant Dermatologist, Vadodara Code Number: dv08101 Abstract Median canaliform deformity of the nail is an uncommon entity, where there is longitudinal splitting of the nail. Longitudinal splitting of the nail is a rare phenomenon and can also occur following number of growths arising in the nail matrix. On examination there was a longitudinal split in the nail plate, beginning in the distal nail fold and extending proximally all the way to the proximal nail fold. There was a small, almost indiscernible, swelling in that area, which was exquisitely tender. The split part of the nail showed a little discoloration. There was no discharge, bleeding, or subungual mass visible. 'Love test' was positive in this case. After nail avulsion, a small 2 mm x 4 mm nodule was exposed and excised. Histopathological examination of the tumor showed a mantle of glomus cells surrounding the blood vessels. Keywords: Glomus tumor, Longitudinal splitting of nail, Median canaliform dystrophy Introduction Longitudinal splitting of the nail as seen in median canaliform dystrophy is most commonly reported following chronic trauma. However, underlying tumors of the matrix can also cause longitudinal splitting. An interesting case of glomus tumor of the nail causing a longitudinal splitting of the nail, resembling median canaliform dystrophy, is being reported.Case History A 72-year-old Spanish missionary reported to this clinic with an exquisitely painful left thumb nail, which was also split in the center. He said that he had developed this split a couple of years ago; when he also noticed pain, which gradually became more intense. The longitudinal split in the nail also grew during that period. He complained of severe pain even when his finger touched a hard surface. There was no history of drug intake or any family history of a similar affliction. There was no history of any repeated trauma or any habit tic involving manipulation of the nail apparatus. On examination there was a longitudinal split in the nail plate, beginning in the distal nail fold and extending proximally all the way to the proximal nail fold [Figure - 1]. There was a small, almost indiscernible, swelling in that area, which was exquisitely tender. The split part of the nail showed a little discoloration. There was no discharge, bleeding, or a subungual mass visible. ′Love test′ was positive in this case, i.e., pressure applied over the lesion with the tip of a pencil eliciting excruciating pain. A provisional diagnosis of longitudinal nail splitting mimicking median canaliform dystrophy of the nail due to an underlying glomus tumor was made. The nail plate was avulsed, and the nail bed and matrix were explored. A small bluish nodule measuring about 2 mm x 4 mm was seen in the matrix. The tumor was excised and the site was sutured. Histopathological examination of the tumor showed a mantle of glomus cells surrounding the blood vessels [Figure - 2]. The cells were rounded and uniform, with eosinophilic cytoplasm and round-to-oval nuclei. The stroma at places was conspicuously myxoid. There were no features of cellular or nuclear pleomorphism. A diagnosis of glomus tumor was made. The longitudinal split in the center of the nail, mimicking median canaliform dystrophy of the nail, was logically assumed to be secondary to the glomus tumor. Discussion Median canaliform dystrophy of Heller (dystrophia unguis mediana canaliformis, solenonychina, nevus striatus unguis), as the name suggests, is a dystrophic condition of the nail in which longitudinal splitting occurs. [1] It is almost exclusively seen on the thumbs, and often there is bilateral involvement of thumbnails. In most cases, there is a fir-tree pattern, which was not seen in this case. [1] Repeated trauma, especially manipulating the central part of the cuticle, has been implicated in this disorder. However, it is not seen uniformly in all cases of median canaliform deformity of the nail. [1],[2],3] There can be waxing and waning or persistence of the lesion despite many years of scrupulous avoidance of any trauma. That questions the widely supported belief that the entity is secondary to chronic trauma. [4] Isolated cases of its association with isotretinoin therapy and a familial occurrence have been reported. [5],[6] Benign and malignant tumors like glomus tumor, myxoid cyst, papilloma, squamous cell carcinoma, malignant melanoma, etc., can have a subungual location and can cause nail dystrophy, including longitudinal grooving and lifting of the nail plate from the bed. [1],[3] It is suggested that glomus tumors should always be kept in mind when considering differential diagnosis of any painful condition of the terminal digit. [7] Subungual solitary glomus tumors (neuromyoarterial tumors) can either be skin colored or bluish. They are usually extremely tender, and there can be constant severe pain which radiates upon touch or change in temperature. [7],[8],[9] They can also cause concave surface erosions of the underlying bone, seen by a plain x-ray. Histopathologically, they are characterized by cuff of uniform glomus cells surrounding vascular lumina. [10] The vascular lumina may either be inconspicuous or be very prominent to merit the appellation of glomangioma. There may be a transition from glomus cells to smooth muscle cells too, which is when it is known as glomangiomyoma. In addition to these features, some glomus cell tumors show abundant myxoid stroma, which was true for this case too. [10] A complete excision is indicated for relief of pain; however, when present in subungual location, their small size makes them difficult at times to be located and eradicated. [1],[11] In our case too, one small tumor measuring 2 mm x 4 mm was not visible until the nail was avulsed. A glomus tumor induced longitudnal splitting of the nail resembling a medial canaliform deformity of the nail without the fir tree pattern is being reported. Acknowledgment I thank Dr. Mayur Jani, plastic surgeon, for the surgical intervention. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08101f2.jpg] [dv08101f1.jpg] |
| |||||||||

{kind=link}
{kind=link}