 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
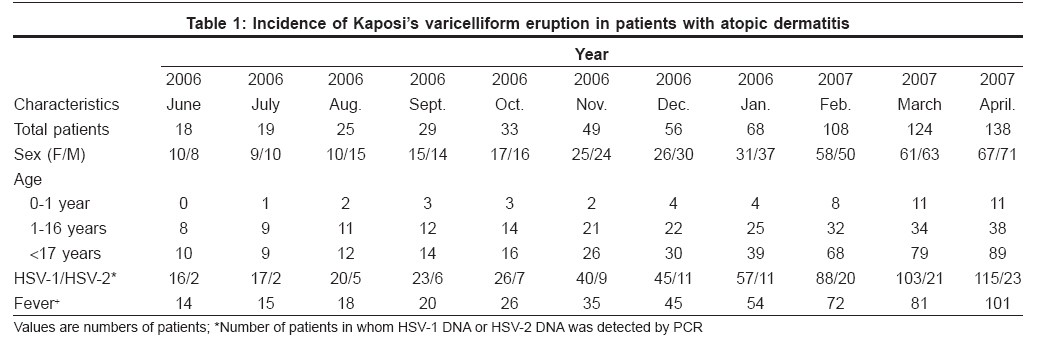
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 260-261 Letter To Editor Rapidly increasing incidence of Kaposi's varicelliform eruption in patients with atopic dermatitis Kimata Hajime Department of Allergy, Moriguchi-Keijinkai Hospital, 2-12-47, Moriguchi City, Osaka Prefecture Code Number: dv08102 Sir, Kaposi′s varicelliform eruption (KVE) is occasionally observed in patients with atopic dermatitis (AD). [1] However, most of them are sporadic cases and no detailed analysis of the monthly incidence of KVE has been reported with accurate diagnosis by PCR. We analyzed the incidence of KVE in our hospital since the year 2006. All of the patients had typical features of AD. KVE was diagnosed clinically based on the appearance of disseminated vesicles, pustules or erosions on face and various other sites of the body. Skin swabs taken from the lesion according to a previous report, demonstrated the presence of HSV-1 or HSV-2 DNA by PCR. [2] Patients in whom HSV-1 or HSV-2 DNA was not detected by PCR, were excluded. As shown in [Table - 1], monthly incidence of KVE was less than 20 cases in June 2006 or July 2006. Similar numbers were seen in previous years in our hospital. However, the incidence began to increase in all ages since August 2006 and it reached 138 cases in April 2007. The youngest patient was a 2.5 month-old baby. HSV-1 was detected in most of the cases while HSV-2 was detected in only a few cases. Children (< 16 years of age) were treated with oral acyclovir (20 mg/kg) four times a day and vidarabine ointment for 7-14 days. On the other hand, adults (>17 years of age) were treated with valacyclovir 1000 mg three times a day and vidarabine ointment for 7-10 days, except for 20 patients who were admitted to hospital and treated with intravenous acyclovir 250 mg three times a day for 7-10 days. Antibiotics were administered when patients had secondary bacterial infection. After treatment, skin lesions healed completely in all of the patients. The reasons for the rapidly increasing incidence of KVE remain to be elucidated. It was reported that a mini-outbreak of KVE occurred in a skin ward. [3] However, the outbreak of herpes infection in a local area was an unlikely explanation as patients came to our hospital from various cities in Japan. Moreover, the incidence of herpes infection in subjects without AD was not found to be increased in our hospital. It was reported that risk factors for KVE were the reduced production of some cytokines (IFN-β or CXCL 10/IP-10) or elevated serum total IgE levels. [4] In fact, serum total IgE levels in KVE patients younger than a year of age (338 + 22 IU/ml, n = 48) were significantly higher than those in age-matched AD patients without KVE (157 + 8 IU/ml, n = 48). Large scale analysis will be necessary to survey the worldwide incidence of KVE. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08102t1.jpg] |
| |||||||||

{kind=link}