 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
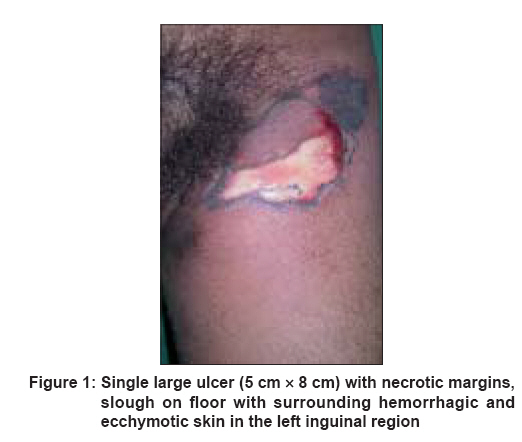
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 268-270 Letter To Editor Necrotizing fasciitis in an HIV-infected patient Surjushe Amar, Vasani Resham, Thakre Minal, Saple DG Department of Dermatology, Venereology and Leprosy, Grant Medical College and Sir JJ Group of Hospitals, Mumbai Code Number: dv08109 Sir, Necrotizing fasciitis is a life-threatening, progressive, rapidly spreading, inflammatory infection of the deep fascia, with secondary necrosis of the subcutaneous tissues and usually associated with the trauma and immunodeficiency. We present a case of necrotizing fasciitis in an HIV-infected patient. A 27-year-old unmarried male presented with painful raw lesions over the left inguinal region since 3 days. It started with a painful left inguinal swelling associated with high-grade fever followed by the formation of blisters, which ruptured spontaneously to form raw lesions. He was non-diabetic and gave no history of trauma or invasive procedure. On examination, there was a single large ulcer with necrotic slough on the floor, irregular edges, and the surrounding skin showing ecchymosis [Figure - 1]. A differential diagnosis of cutaneous vasculitis, necrotizing fascitis, pyoderma gangrenosum, and pyomyositis was entertained and the patient was investigated. His hemogram, liver function tests, renal function tests, electrocardiogram, coagulation profile, and X-ray chest were normal. Erythrocyte sedimentation rate was 30 mm at the end of one hour and ELISA for HIV-I was positive. Pus culture grew beta hemolytic streptococci and Pseudomonas aeruginosa . Blood culture was normal and CD4 count was 350 cells/ml. Sonography of the abdomen showed external iliac lymphadenopathy and mild splenomegaly. Anti-nuclear antibody and pathergy test were negative. On histopathology, there was a dense infiltrate of polymorphonuclear cells in the dermis and subcutaneous tissue mostly around the blood vessels. Surgical debridement was done and he was started on injectable cefotaxime (1 gm iv 8 hrly), amikacin (500 mg iv 12 hrly), and metronidazole (500 mg iv 8 hrly) along with daily dressing. Split-thickness skin grafting was done with significant healing in 2 weeks′ time [Figure - 2]. Necrotizing fasciitis was first described by Wilson. [1] Hospital gangrene, progressive bacterial synergistic gangrene, Fournier′s gangrene, streptococcal gangrene, and flesh-eating bacterial infection are the other terms used. It is of two types, depending on the organisms isolated. Type 1 is polymicrobial, usually caused by aerobic and anaerobic organisms, while Type 2 is caused by Group A β -hemolytic streptococci, either almost always alone or in combination with other species. [2] Our case was of Type 2. The organism enters into the subcutaneous space through a disruption of the overlying skin either by trauma or surgery, or lympho-hematogenous spread from a distant site, but rarely infection can occur over healthy skin. [3] Necrotizing fasciitis has reported cumulative mortality of 34%, with the range being 6 to 76%. [4] In suspected necrotizing fasciitis, a full-thickness biopsy, particularly if combined with more extensive surgery, has been shown to correlate with an improved outcome. [5] Clinical suspicion of necrotizing fasciitis should be high because early diagnosis and early treatment, including wide excision and debridement, along with antibiotics decrease patient morbidity and mortality in this otherwise poorly-prognostic condition. [6] In immunocompromised host, particularly, it becomes mandatory to biopsy any necrotic cellulitic lesions and to be alert to the possibility of a wide range of bacterial, viral, fungal, and even parasitic infestations. [2] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08109f2.jpg] [dv08109f1.jpg] |
| |||||||||

{kind=link}
{kind=link}