 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
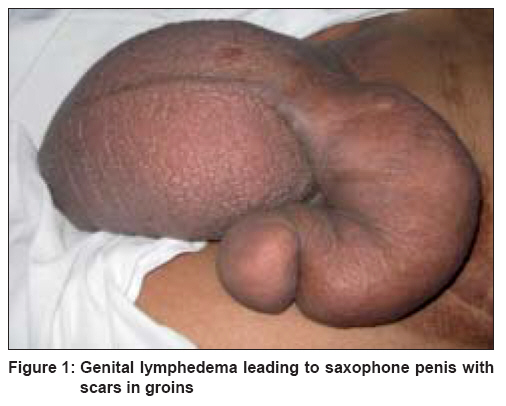
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 270-271 Letter To Editor Unusual cause of saxophone penis Vaishampayan Sanjeev Department of Dermatology, 155, Base Hospital, C/O 99 APO, 901213 Code Number: dv08110 Sir, Lymphedema is the occurrence of chronically swollen extremities or rarely the genitals due to inadequate drainage of interstitial fluid by the lymphatics. Primary lymphedema is uncommon and has female predominance. It may be congenital or familial (Milroy′s disease) or idiopathic appearing either at puberty (precox), or after 35 years of age (tardum). [1],[2] Secondary lymphedema caused by obstruction of lymphatic flow due to destruction of lymphatics by various infections is relatively common. In India, secondary lymphedema is synonymous with filariasis. [1] Other causes include surgical removal of lymph nodes or their destruction by radiation fibrosis and malignant cell infiltration. [2] Genital elephantiasis though uncommon is an important medical problem occurring in the tropics. It causes not only a major physical disability, but also extreme mental anguish. In the majority, filariasis is the cause but bacterial sexually transmitted infections (STIs) like lymphogranuloma venereum and donovanosis form a significant number. Other causes of genital elephantiasis like infections and malignancies are very rare. [3],[4] A 45-year-old man, father of four, with swelling of scrotum and penis of about 2 months duration was referred by a surgeon. Onset was sudden and within 2 weeks he developed a large swelling of penis and scrotum. He only had a feeling of heaviness and was depressed due to the embarrassing condition. There was no history of injury, operation, or radiation prior to the onset. He had a large number of pus-filled eruptions on both legs with fever, about 8 weeks prior to the onset. He was treated by a doctor (non-dermatologist) with oral and topical antibiotics. All lesions had healed in 10-15 days leaving behind scars. There was no history of extramarital sexual contact or genital ulcer disease. His wife was apparently healthy. Clinically, he did not have lymphadenopathy. General and systemic examinations were essentially normal. Genital examination revealed a cold, non-tender, large-curved penis measuring 8 inches in length and 5 inches in circumference, looking like a "saxophone" [Figure - 1]. There was no evidence of ulcer, scar, or inflammation. The scrotum was huge and its contents could not be palpated. Both weighed about 1.0 kg. Transillumination test of scrotal swelling was negative. Left side of his lower abdomen and adjacent area of left thigh had extensive postburn scars, but no edema. Both shins and legs had large number of scars without any sign of inflammation. On the basis of history and clinical findings, a diagnosis of secondary lymphedema of penis and scrotum with "saxophone" deformity was made. In this case, genital lymphedema was secondary to bacterial infection, probably due to Staphylococcus aureus , but peculiarly the lymphedema of genitalia was proximal to the site of infection, i.e. legs and thus was very unusual. Though he had a large scar over inguinal region and lower abdomen due to burns in childhood, it was highly unlikely to be the cause since it happened nearly 35 years back. Absence of suggestive history, genital ulceration and inguinal lymphadenopathy ruled out STIs as a cause for the lymphedema. All relevant hematological and biochemical tests (including repeated night peripheral blood smears for microfilariae, erythrocyte sedimentation rate, serum Venereal Disease Research Laboratory (VDRL) test, and ELISA for HIV (enzyme linked immunosorbent assay for human immunodeficiency virus) were normal. Noninvasive screening for malignancy did not reveal any findings. Lymphangiography was not resorted to due to peculiar site and its inherent complications. He was initially treated empirically with diethylcarbamazine 200 mg tds by a surgeon without any response. Later he was given doxycycline 100 mg BD for 21 days with anti-inflammatory drugs, but did not show much of improvement. Other conservative methods like graduated compression/stockings or infiltration of 5,6 benzo-alpha-pyrone (coumarin) were not possible because of the peculiar site. He was very depressed and had a feeling of shame hence after counseling the patient was referred for surgical management. Secondary lymphedema is relatively common and is caused by various infections. STIs like LGV and donovanosis are causative factors in a significant number of cases. Other causes of genital elephantiasis are very rare and include infections (due to coagulase positive staphylococci, hemolytic streptococci, and tuberculosis) and malignancies. [3],[4] Even if these organisms cannot be cultured, therapy should be directed toward these infections, as was done in our case. Drugs like doxycycline if given for prolonged period may be effective due to additional anti-inflammatory properties. [3] Lymphedema is usually insidious, painless and occurs distal to the site of involvement and may include the site itself. However, in our case genital lymphedema occurred proximal to the site of infection (legs). Long-standing cases develop "elephantiasis nostras verrucosa." However, very rarely lymphangiosarcoma or recurrent episodes of cellulitis and lymphangitis may occur, thus aggravating lymphedema. [1] This necessitates prompt treatment. In case medical and conservative management fails, surgical treatment becomes imperative. Genital elephantiasis is a functionally disabling and emotionally incapacitating entity. It causes extreme discomfort due to weight with limitation in ambulation and difficulty in maintenance of local hygiene and interferes with sexual intercourse. These functional disabilities cause extreme emotional stress making surgical intervention imperative. [5] Various methods of reconstruction of genital elephantiasis involve excision of affected tissue and its reconstruction with or without lymphangioplasty. Out of the several procedures described in the literature, modified Charles procedure looks most promising. These surgical procedures if performed well give remarkably good cosmetic results with tremendous improvement in quality of life of these unfortunate patients with genital elephantiasis. [5] This case is unique due to its rare cause, viz. infection with pyogenic bacteria distal (legs) to the site of involvement. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08110f1.jpg] |
| |||||||||

{kind=link}