 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
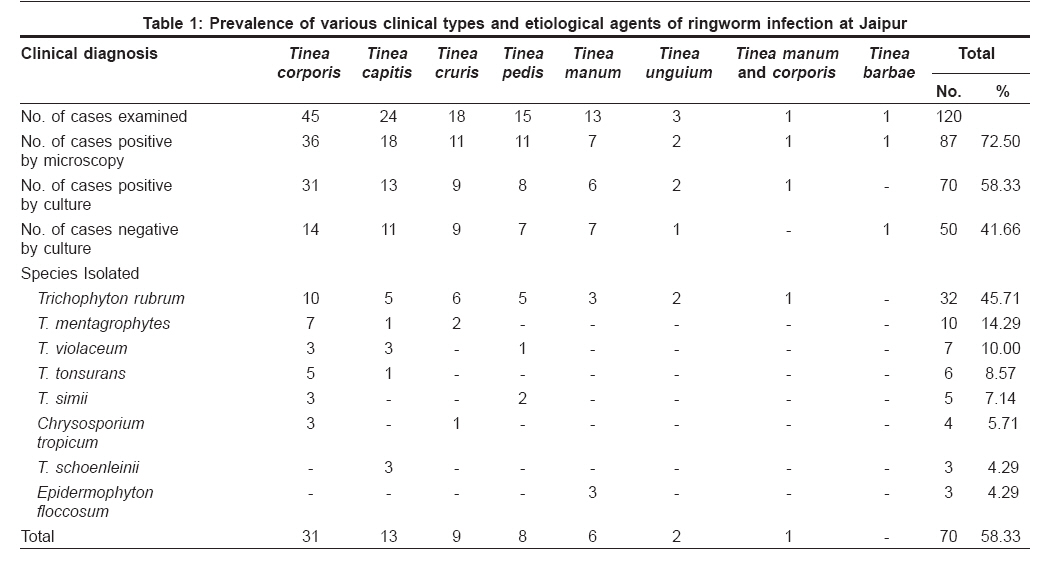
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 274-275 Letter To Editor Clinico-mycological profile of dermatophytosis in Jaipur, Rajasthan Jain Neetu, Sharma Meenakshi, Saxena VN Department of Botany, Laboratory of Microbiology and Mycology, University of Rajasthan, Jaipur, Rajashthan Code Number: dv08114 Sir, Jaipur has got a dry climate but in the summer, the temperature exceeds even 46°C with high humidity during the monsoon season. These climatic conditions favor the occurrence of fungal infections. To determine the clinical features and causative agent of dermatophytosis in the Jaipur area, a study was conducted over six months in the Skin Outdoor Patients Department, SMS Hospital, Jaipur. Clinical samples from 120 patients were subjected to potassium hydroxide (KOH) examination and culture isolation. Sabouraud′s dextrose agar (SDA) medium was used for the isolation, purification and maintenance of dermatophytes. Causative agents were identified microscopically. Out of 120 diagnosed cases, 87 were found to be positive by KOH examination and 70 were culture-positive cases. Thus, the diagnosis of dermatophytosis could be established in 58.33% of the cases examined. In our present investigation, Trichophyton rubrum was the most predominant etiological agent reported from 32 cases (45.71%)[Table - 1]. It was isolated from all clinical types except tinea barbae. A review of the literature for dermatomycoses occurring in India and other countries also corroborated our finding that T. rubrum was the prevalent species. [1],[2],[3] George [4] has suggested that both the predominantly chronic nature of the infection and the adaptation of the dermatophyte to the human skin can explain the higher predominance of T. rubrum in India. The increased virulence in the Indian strains of all dermatophytes resulted from frequent human physical contact, which leads to favorable conditions for parasitism. The second-most common species was found to be T. mentagrophytes (14.29%), followed by T. violaceum (10%), T. tonsurans (8.57%), T. simii (7.14%), and Chrysosporium tropicum (5.71%). T. schoenleinii (4.29%) was isolated for the first time from skin scrapings from Jaipur patients but only in cases with tinea capitis infection. In the present investigation, tinea infections were more common in the 31-40 (23.33%) followed by 1-10 (22.5%), 21-30 (19.17%) and 11-20 (17.5%) age groups. Tinea corporis was the most predominant clinical type reported in all age groups but a higher incidence was observed in the 21-30 and 31-40 age groups. Similar results were also obtained by various other authors. [2],[5],[6] Tinea capitis was the second-most common clinical type reported only in the 1-10 and 11-20 age groups. It may be assumed that a higher freedom of movement, carelessness and perhaps, lack of guidance regarding personal hygiene could be the factors in exposing students to a higher incidence of tinea infection mainly by tinea capitis. It was also noted that patients of higher age groups were less frequently affected. Tinea infections were more dominant in males (67.5%) than in females (32.5%) of all age groups except in the 0-10 years age group where the percentage of female (12.5 vs 10% males) patients was greater. Philpot [7] suggested that males may be more vulnerable to infection due to the higher exposures in the army, school and sporting activities and due to the types of shoes and socks used. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08114t1.jpg] |
| |||||||||

{kind=link}