 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
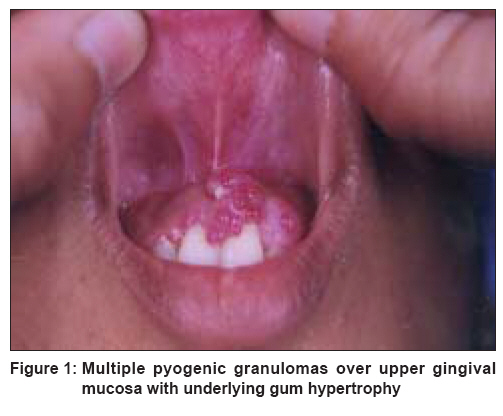
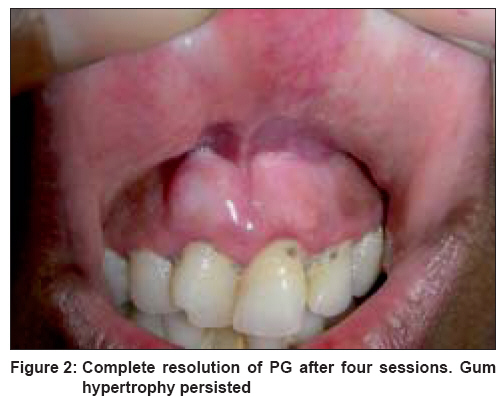
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 275-277 Letter To Editor Successful treatment of multiple gingival pyogenic granulomas with pulsed-dye laser Khandpur Sujay, Sharma VinodK Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi Code Number: dv08115 Sir, Pyogenic granuloma (PG) is a common, usually solitary, lobulated, benign vascular proliferation of the skin and mucous membranes, presenting as hemorrhagic, sessile or pedunculated growth, especially in children and women of reproductive age. Multiple PGs, developing either spontaneously or secondary to trauma, skin inflammation, or systemic immunosuppression are rarely seen. [1],[2] There are only a few reports that highlight the therapeutic success of flashlamp tunable pumped pulsed dye laser (PDL) in multiple mucocutaneous PGs. [3],[4] We report a case of multiple PGs involving the upper gingival mucosa which was successfully treated with PDL without any significant complications. A 38-year-old woman presented with multiple, reddish nodules on the upper gingiva and upper lip, which bled profusely on trauma, since 3.5 years. A year before this, similar lesions around the nose had been excised. There was no history of dental manipulation or immunosuppression. She had no systemic complaints. Dermatological examination revealed approximately 14, 1-2 mm sized, reddish, sessile nodules on the upper gingiva and corresponding labial mucosa [Figure - 1]. Underlying gum hypertrophy was present. Histopathology was consistent with PG. Routine hematological, biochemical, and serological investigations were normal. Enzyme-linked immunosorbent assay (ELISA) for human immunodeficiency virus (HIV) and Venereal Disease Research Laboratory (VDRL) test were nonreactive. Computed tomography (CT) of the paranasal sinuses revealed right-sided maxillary sinusitis. The lesions were treated with the tunable pumped PDL (Photogenica Cynosure VLS, Chelmsford, MA, USA). The laser parameters used were: spot size - 5 mm, fluence - 6-7.5 J/cm 2 (at purpuric threshold), wavelength - 585 nm, pulse duration - 450 ms. Local anesthetic (2% lignocaine) was infiltrated before the procedure. The laser therapy was repeated every 4 weeks. Pulses were administered in an overlapping manner (4-5 pulses per lesion). There was partial resolution of the PG after two sessions. All the lesions subsided after four sessions [Figure - 2]. There was no scarring. However, underlying gum hypertrophy persisted. During the next 6 months, two new lesions appeared on the right upper gingival and one in the labial mucosa. In this report, we seek to highlight the therapeutic success achieved with PDL in multiple mucosal PGs. There are only anecdotal reports of successful treatment of mucosal PG with PDL. [4] Multiple eruptive PGs involving the trunk, limbs, oral mucosa, penis, labia majora, and sigmoid colon, have been reported. [1],[2],[5],[6],[7],[8] They appeared either spontaneously or secondary to trauma, burns, surgical manipulation by excision, cauterization and curettage, oral PG developed around dental implants or in association with pregnancy while other lesions occurred in association with exfoliative dermatitis, systemic retinoid therapy, and immunosuppressive disorders like Hodgkin′s disease, hypogammaglobulinemia, allogenic bone marrow transplant, alcoholic cirrhosis, malignancy, decreased helper/suppressor T-cell ratio, and low interleukin 2 levels. [1],[2],[3],[4],[5],[8] In our patient, there was history of surgical excision in the nasal area prior to development of these lesions. Laser therapy using continuous and pulsed CO 2 and Nd:YAG systems have been undertaken for a variety of intraoral soft tissue lesions such as hemangioma, lymphangioma, squamous papilloma, lichen planus, focal melanosis, and PG, since they carry the advantage of being less invasive and sutureless procedures that produce only minimal postoperative pain. [9] PDL has shown excellent results in cutaneous PG with only minimal pigmentary and textural complications. [10] Gonzales et al , demonstrated both symptomatic and clinical clearing of the lesions with excellent cosmetic results in 16 of 18 treated patients. [10] However, there is minimal convincing proof of its efficacy in intraoral PG. [4] We achieved complete resolution of multiple PG located on the upper gingiva and labial mucosa after four sessions with PDL, without producing any complications. There was no scarring. Only three lesions recurred during the next six months. Hence, PDL may be a good therapeutic option for multiple intraoral PG. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08115f2.jpg] [dv08115f1.jpg] |
| |||||||||

{kind=link}
{kind=link}