 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
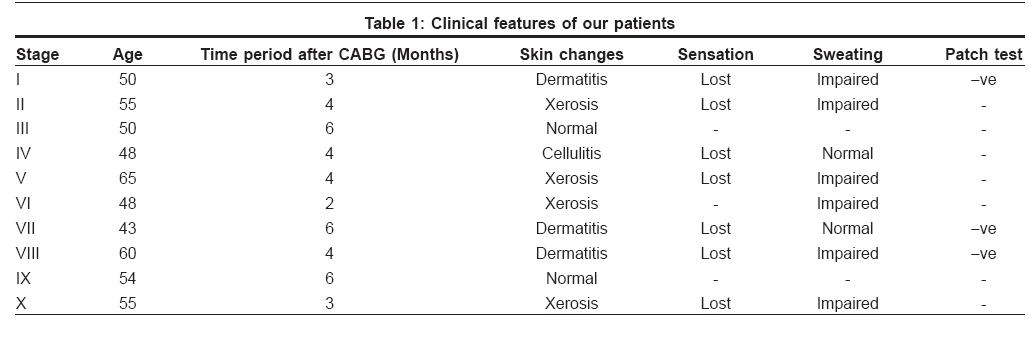
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 278-279 Letter To Editor Saphenous vein graft dermatitis in patients with coronary artery bypass graft Rai Reena, Srinivas CR, Vardharaj K Department of Dermatology, PSG Hospitals, Peelamedu, Coimbatore, Tamil Nadu Code Number: dv08117 Sir, Coronary artery bypass grafting (CABG) is the most frequently performed cardiac surgical procedure in the world. Along with the internal mammary and radial arteries, the greater saphenous vein (SV) is a commonly used conduit in CABG. The incision required for the removal of the SV has been 30-45 cm long and may at times extend from the thigh to the ankle. As a result, the harvest of the SV is commonly associated with pain, discomfort, scarring, and the increased risk of wound infection. [1] There are reports of dermatitis and anesthesia at the site of SV graft scars. [2] Due to alteration in the integrity of skin, there is an increase in morbidity in these patients. We examined the local changes over SV graft donor site in 10 patients who underwent CABG. Ten male patients who underwent CABG were examined. All patients were between the age groups of 45 and 60. We included all patients who have undergone CABG in whom SV has been removed from one leg. Patients with preexisting dermatitis, varicose eczema, leg ulcers, peripheral neuropathy, or with preexisting loss of sensation over the lower leg were excluded from the study. These patients were examined and the findings were recorded. Sensations were tested and sweat test with ninhydrin was performed on all patients. [3] Patch testing was performed using standard series on patients with suspected contact dermatitis and other relevant antigens namely topical applications used by the patients were also patch tested. The results of the skin changes are tabulated in [Table - 1]. In all patients, scars were seen extending from mid-thigh to ankle. Eight out of ten patients had anesthesia at the site of the scar, one had cellulitis, three had dermatitis, and four had xerosis. There was no relationship between the length of incision, time after surgery, and dermatitis. All patients with dermatitis responded to topical steroids and emollients. One patient complained of associated pruritus while in the others the dermatitis was asymptomatic. The sweating was impaired in six patients and patch tests on patients with dermatitis did not show any positive results. Cutaneous complications following SV harvesting for CABG may result in alteration in skin integrity resulting in significant morbidity. [2] These changes are possibly due to the long incisions made over the skin for harvesting the graft. The surgery possibly results in damage to the blood vessels, lymphatics, and nerves. This leads to reduced blood supply both to the skin as well as to the nerves resulting in loss of sensation and autonomic changes such as dryness, loss of sweating. Cellulitis, [4] nonhealing ulcers, [5] painful peripheral sensory neuropathy [6] and vein graft dermatitis, [2] have all been reported. Trophic changes of the skin have been seen in association with disease or injury to peripheral nerves and have been termed trophoneuroses. We too report similar findings. After denervation, motor, sensory, and autonomic functions may be disrupted resulting in xerosis, loss of sweating, loss of sensation, loss of barrier function predisposing to dermatitis, and infection. Although most patients accept this as a smaller trade off, CABG is being increasingly done and measures to either prevent or minimize the complications are justified. An approach to patient management including treatment of the dermatitis with topical corticosteroids and emollients, education regarding possible exacerbating factors and immediate treatment of the complications will help reduce morbidity in patients. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08117t1.jpg] |
| |||||||||

{kind=link}