 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
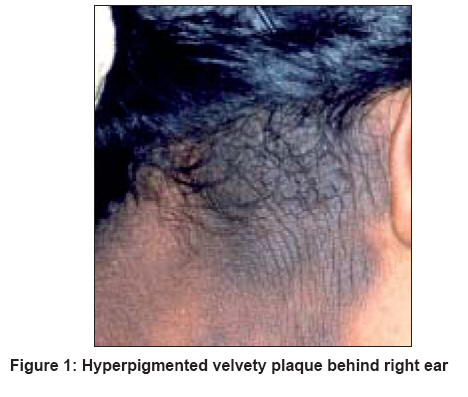
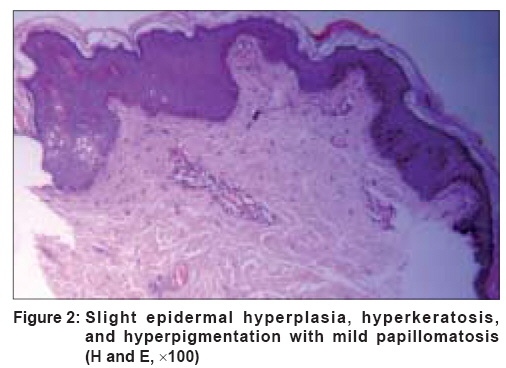
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 279-280 Letter To Editor Nevoid acanthosis nigricans Das JayantaKumar, Sengupta Sujata, Gangopadhyay Asok Department of Dermatology, Vivekananda Institute of Medical Sciences, Ramakrishna Mission Seva Pratisthan, Kolkata, West Bengal Code Number: dv08118 Sir, Acanthosis nigricans (AN) is usually a symmetric eruption characterized by a hyperpigmented, velvety cutaneous thickening that can occur on any part of the body, but characteristically affects the axillae, nape and the sides of the neck, the groin, antecubital and popliteal surfaces, and umbilical area. [1] It is a cutaneous marker, most frequently of insulin resistance and less frequently of malignancy. [2] Nevoid AN is a rare form of AN that manifests at any age at or before puberty and has a morphologic pattern similar to other forms of AN. [3] It is not associated with syndromes, endrocrinopathies, drugs, or malignancies. [3],[4] It is said to be inherited as an irregularly autosomal dominant trait that may first become evident at birth, in childhood, or during puberty. [3] Nevoid AN classically extends for a certain period and then either remains stationary or starts regressing. [1],[3] Benign AN and benign inherited AN, are the names proposed by some authors for the same disorder. [1],[5] Unilateral nevoid AN is another term that has also been used to denote this entity. [3] A case of nevoid AN is reported here as the condition was rarely reported from India and in world literature. An 18-year-old girl presented with a localized area of nonpruritic thickened and pigmented skin on right side of the nape of the neck for 7 years. The first-born among three children born to nonconsanguineous parents, she did not have any other member of her family affected with similar lesions [Figure - 1]. It started as a small brown asymptomatic papule a little behind the right ear, and gradually spread to the present size in a span of 3 years, and then stopped growing further. There was no history of rubbing the area. On dermatological examination, a brown black velvety plaque with soft ridges, measuring about 7 cm ´ 5 cm, was seen. The borders were irregular with the affected skin gradually merging imperceptibly with normal skin. The skin was otherwise normal. Palms and soles, mucous membranes, genitals, hair, and nails were normal. The patient was non-obese, with a body mass index (BMI) of 20.1, and systemic examination was unremarkable. Complete blood count and routine urine analysis were within normal limits. Venereal Disease Research Laboratory (VDRL) test was nonreactive. Fasting blood sugar was 87 mg/dl and postprandial blood sugar was 108 mg/dl. Fasting insulin level was 11.3 IU/ml. The hepatic enzymes, T3, T4, TSH, and growth hormone were within normal range. Radiographic examination of the chest, skull, and hands were normal. Abdominal ultrasonography was normal. Biopsy of the skin showed hyperkeratosis, papillomatosis, increased pigmentation of the basal cell layer, and mild acanthosis, with a sparse inflammatory infiltrate of mononuclear cells in the upper dermis [Figure - 2]. Nevoid AN has been grouped together with "syndromic AN" and "acral acanthotic anomaly" under the heading "other" causes of AN in a recent classification of AN. [2] Nevoid AN is said to have resemblance to ichthyosis hystrix and confluent reticulate papillomatosis, but in this case they could be clinically ruled out. Differentiation from linear epidermal nevus and from the hyperkeratotic type of seborrheic keratosis is more difficult, and it has even been suggested that this form of AN can be classified as a type of epidermal nevus so far as the histogenesis of this lesion is concerned, although its status as a distinct clinical and histopathological entity is recognized. [5] However, in this case seborrheic keratosis could be ruled out clinically. Linear epidermal nevus, which shows more marked acanthosis and has a more compact orthokeratotic stratum corneum, was ruled out histologically. In view of the fact that nevoid AN is considered an irregularly autosomal dominant trait, the absence of family history is noteworthy. [3] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08118f2.jpg] [dv08118f1.jpg] |
| |||||||||

{kind=link}
{kind=link}