 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
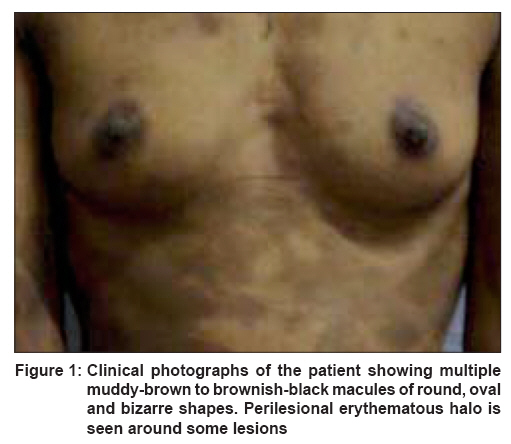
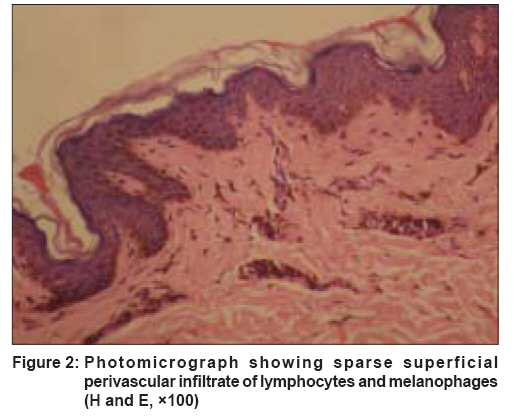
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 281-282 Letter To Editor Ashy dermatosis-like pigmentation due to ethambutol Srivastava Neeraj, Solanki LakhanS, Chand Satish, Garbyal RajendraS, Singh Sanjay Department of Dermatology, Institute of Medical Sciences, Banaras Hindu University, Varanasi Code Number: dv08119 Sir, A 30 year-old Indian woman presented to us with asymptomatic, multiple, hyperpigmented macules. She had been receiving treatment for abdominal tuberculosis in the form of levofloxacin (750 mg daily) and ethambutol (800 mg daily) for two months, followed by levofloxacin, rifampicin (450 mg daily) and isoniazid (300 mg daily) for eight months. Macular lesions appeared on her forearm about two weeks after starting the initial treatment course. No new lesions had appeared and existing lesions did not enlarge since ethambutol was stopped; however, the pigmentation had persisted. Multiple, non-scaly, slightly atrophic, muddy-brown to brownish-black macules of round, oval and bizarre shapes and different sizes (0.5-10 cm in size) were present over the face, neck, upper extremities and the trunk [Figure - 1]. Some of the lesions, especially those on the abdomen, had perilesional erythematous halos. Palms, soles, scalp and mucosal surfaces were unaffected. Routine investigations were normal. Histopathological examination showed mild epidermal atrophy with a slight flattening of rete ridges and a sparse superficial perivascular infiltrate of lymphocytes. Papillary and deep dermis showed numerous melanophages [Figure - 2]. These findings were consistent with ashy dermatosis. Ashy dermatosis (erythema dyschromicum perstans) is an asymptomatic eruption of oval, polycyclic or irregularly shaped, grey-blue, hyperpigmented macules on the trunk, arms, face, and the neck. [1] It begins as ash-coloured macules, sometimes with an erythematous or elevated border. The oral cavity and genitals are spared. It has been associated with ingestion of ammonium nitrite, orally administered radiographic contrast media and whipworm infestation. [1] Ethambutol has only rarely been reported to cause lichenoid eruptions; [2],[3] however, it has never been reported to cause ashy dermatosis-like eruptions. In one report of ethambutol-induced lichenoid eruption, the eruption consisted of lichenoid papules, [2] while another report described the eruption consisting of lichenoid papules and hyperpigmented macules. [3] Some authors believe that ashy dermatosis may be a manifestation of lichen planus. [1] The present case appears to be the first in which ethambutol most probably led to ashy dermatosis-like pigmentation. We believe that the pigmentation in the present case may be better called ashy dermatosis-like rather than lichenoid, because of the presence of a perilesional, inflammatory, erythematous halo and inconsistent basal cell degeneration. A challenge test with ethambutol was considered unethical. Re-exposing a patient with a drug eruption to the suspected drug may be dangerous, and hence, is not usually recommended. [4] The time course of eruption strongly suggested that ethambutol was responsible for the eruption. Sometimes, the issue as to whether a particular drug is really responsible for an eruption, is debatable. Although no perfect solution exists, the Naranjo adverse drug reaction probability scale is frequently used to clarify this issue. [5] In the present case, the likelihood of ethambutol causing the eruption was considered to be probable, which is one step below the highest certainty provided by this scale. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08119f1.jpg] [dv08119f2.jpg] |
| |||||||||

{kind=link}
{kind=link}