 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
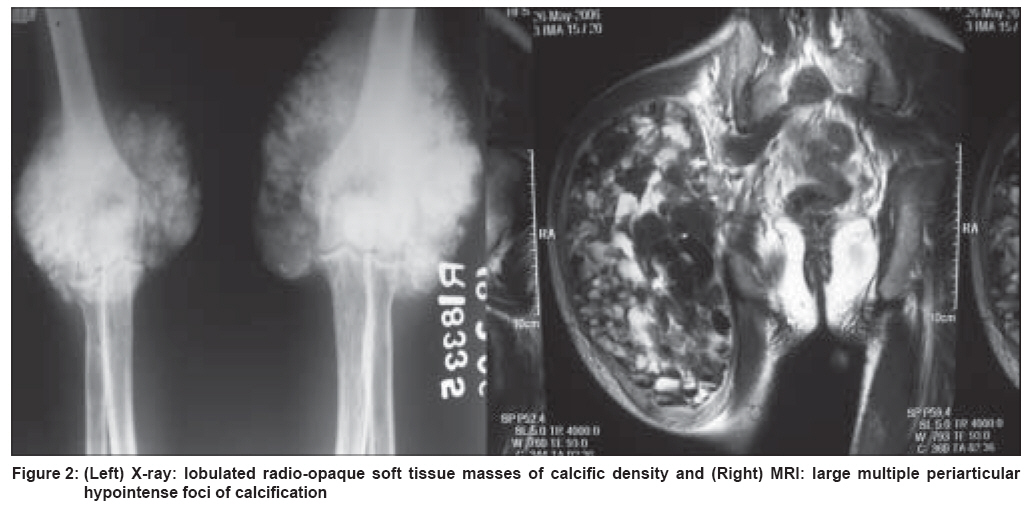
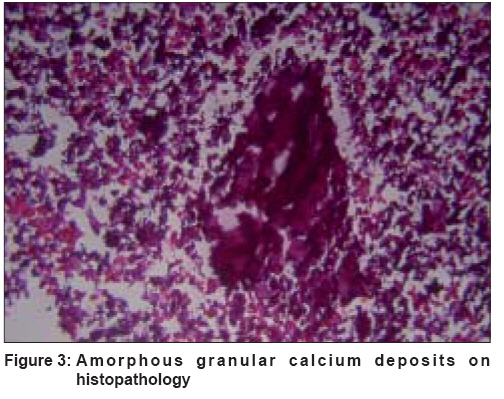
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 282-283 Letter To Editor Tumoral calcinosis Jindal Saurabh, Surjushe Amar, Sao Prajct, Saple DG Department of Dermatology, Venereology and Leprosy, Grant Medical College and Sir JJ Group of Hospitals, Mumbai Code Number: dv08120 Sir, Calcinosis cutis, a group of disorders in which calcium is deposited in the skin is of four types: metastatic, dystrophic, idiopathic and intraepidermal calcified nodules. [1] Tumoral calcinosis is a special form of idiopathic calcinosis which affects adolescents and young adults [2] and is characterized by massive subcutaneous deposits of calcium phosphate near the joints such as hips, shoulders, elbows, wrists, feet and hands. The deposits consist of pleomorphic calcium phosphate (hydroxyapatite) crystals. A 26 year-old married male presented with gradually increasing, painless, bony, hard masses over both the elbows and around the right hip joint prevalent since the last two years. There was no history of excessive milk or antacid intake, endocrinal abnormalities, or any history suggestive of any connective tissue disease. There was also no history of any similar condition in the family members. On examination, there were firm-to-hard, nontender, irregular, tumorous masses over the lateral aspect of the right gluteal region measuring 15 x 15 cm, and over both elbows measuring about 10 x 8 cm with overlying skin showing atrophic scars. There was minimal restriction of movements at the joints [Figure - 1]. Systemic examination results were normal. Hemogram, liver and renal function tests, and the erythrocyte sedimentation rate were normal. Serum phosphorus level was 6 mg% (normal range: 2-4.5 mg%). Serum calcium, uric acid, alkaline phosphatase, parathyroid hormone, calcitonin levels were normal. Antinuclear antibodies and the rheumatoid factor were absent. Radiographs showed large, lobulated, radio-opaque, soft tissue masses of calcific density with radiolucent septae in the juxta-articular position of both elbows and the right hip. Magnetic resolution imaging (MRI) of the right hip showed foci of calcification with infiltration into the gluteus medius and quadratus femoris [Figure - 2]. Histopathology from the elbow showed deeply basophilic amorphous granular material surrounded by dense fibrous tissue and infiltration [Figure - 3]. Debulking of the elbow regions was done and the patient is now on regular follow-up to detect any recurrence. Tumoral calcinosis was first described in 1899. [3] The pathogenesis is obscure but the basic defect is thought to be in the proximal renal tubular cell with an elevated renal phosphate reabsorption threshold and increased production of 1, 25-dihydroxyvitamin D. [4] It is classified into three types depending upon the pathogenesis: primary normophosphatemic tumoral calcinosis (NPTC), primary hyperphosphatemic tumoral calcinosis (PHTC) and secondary tumoral calcinosis. [5] Our case is of subtype 2 having hyperphosphatemia with normal levels of serum calcium, parathyroid hormone and alkaline phosphatase. Tumoral calcinosis is often associated with diseases like chronic renal failure, primary hyperparathyroidism, hypervitaminosis D, milk-alkali syndrome, sarcoidosis and massive osteolysis. [5] Typical clinical findings, radiology, fine needle aspiration cytology, and histopathology [3] showing calcification help in the diagnosis. Various treatment modalities like aluminium hydroxide or acetazolamide have been tried but none has been found to be effective. Complete surgical excision has been recommended but recurrences are common. [6] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08120f2.jpg] [dv08120f3.jpg] [dv08120f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}