 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
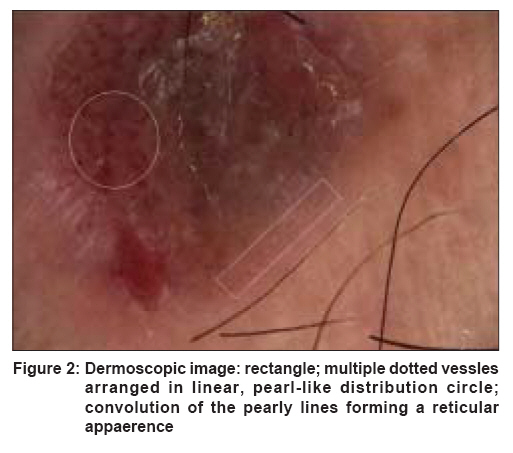
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 285-287 Letter To Editor Clear cell acanthoma: New observations on dermatoscopy Akin FigenYazkan, Ertam Ilgen, Ceylan Can, Kazandi Alican, Ozdemir Fezal Department of Dermatology, Ege University Medical Faculty, Bornova-Izmir Code Number: dv08122 Sir, Clear cell acanthoma (CCA) is characterized by pink-brown nodules with a "stuck-on" appearance or plaques and usually occurs on the legs of elderly people. Dermatoscopy is a noninvasive and a highly valuable method in the diagnosis of pigmented skin lesions and significant improvement has been achieved recently in this method. It is now being used in the diagnosis of nonpigmented skin lesions displaying cutaneous neoangiogenesis. Dermatoscopic features of CCA are not established yet with only a limited number of reports describing it. The common dermatoscopic feature of all these articles is the presence of pinpoint-like/dotted vessels, which are described as having a homogenous/bunch-like, reticular, pearl-like or homogeneous/net-like distribution. Clear cell acanthoma (CCA) was first described by Degos as a benign tumor of epidermal origin. Recently, it has been claimed to be a nonspecific reactive dermatosis. [1] Some authors have also suggested that it is a localized form of inflammatory psoriasiform dermatoses. [1],[2] To our knowledge, only four articles have been presented on the dermatoscopic findings of CCA. [2],[3],[4],[5] The common denominator of all these reports is the presence of pinpoint-like/dotted vessels. [1],[2] A 65 year-old man presented with a 20-year history of a lesion on the posterior aspect of his leg, which darkened and increased in size over the last year. Dermatological examination revealed a red-brown, vascularized plaque with a collarette scaling and central crusting with a diameter of 1 x 1.5 cm on the cruralis posterior [Figure - 1]. Dermatoscopy disclosed multiple dotted vessels arranged partly in a linear, pearl-like distribution [[Figure - 2], rectangle] and partly in a reticular appearance [[Figure - 2], circle] and these were circumscribed by a translucent collarette scaling. Systemic examination of the patient was normal and laboratory tests were within normal limits. Skin biopsy showed micropustules in the upper epidermis, well demarcated epidermal hyperplasia, elongation, fusion and coalescence of the rete ridges. Keratinocytes showed pallor and stained strongly positive with periodic acid Schiff (PAS). CCA is generally characterized with an asymptomatic, slowly growing, single or multiple, pink-brown nodules or small plaques often located in the lower extremities of elderly patients. It has a peripheral collarette of wafer-like scales and a vascularized erythematous component that blanches on pressure. [2] Similarly, our patient displayed a red-brown, vascularized plaque with a collarette of translucent scales localized on his leg over a long period. Irritated seborrheic keratose, basal-cell carcinoma, Bowen′s disease, squamous-cell carcinoma, keratoacanthoma and amelanotic melanoma or nodular melanoma should be considered in the differential diagnosis of CCA,. Dermatoscopically, these lesions can be distinguished by their typical characteristic dermatoscopic features in addition to their vascular structures. Dermatoscopic pattern of CCA was first described by Blum et al. in 2001 as partly homogenous, symmetrically or bunch-like arranged, pinpoint-like capillaries. [3] A similar dermatoscopic pattern was also observed in the psoriatic plaque after removal of the scales. However, these capillaries were seen to display a more homogenous distribution in psoriasis. The authors stated that on dermatoscopy, the distribution of these capillaries corresponded histopathologically to dilated capillaries seen in the elongated dermal papillae in both of them. Nevertheless, they concluded that the dermatoscopic examination was a diagnostic clue and might help to differentiate CCA from other skin tumors. [3] Two years later, Bugatti et al. reported six cases of CCA with psoriasis-like vascular findings on dermatoscopy. [2] It was stated that the dotted, pinpoint-like structures distributed in a reticular pattern were due to dilated capillary loops oriented mainly perpendicularly to the skin surface and at higher magnification, these dotted vessels revealed a bush-like appearance, again with a reticular pattern. The authors reported a squamous surface with translucid collarette as an additional dermatoscopic finding and concluded that this dermatoscopic pattern seemed to be a clue for CCA. [2] In another case described by Zalaudek et al. , it was found that pinpoint or dotted vessels did not display a homogenous distribution throughout the entire lesion as they did in psoriasis. [4] Instead, they appeared in a linear pearl -like distribution as pearls in a line, namely, pearl-like vessels. Hence, they concluded that dermatoscopy of CCA differed from dermatoscopy of psoriasis. [4] Lacarubba et al. reported that symmetric and homogeneous pinpoint-like vascular structures were distributed throughout the entire lesion and tended to be arranged in a net-like pattern which appeared to have a bush-like aspect at higher magnification in 20 CCA lesions. [5] As a result, they concluded that although the dermoscopic pattern was not specific, it might improve the clinical diagnosis of CCA. [5] Our case revealed multiple dotted vessels arranged partly in linear, pearl-like distribution and partly in reticular appearance. These dotted vessels which represent the dilated capillaries oriented mainly perpendicular to the skin surface in the elongated dermal papillae, formed a reticular appearance due to the regular distribution over the surface. Additionally the multiple dotted vessels were circumscribed by a translucent collarette scaling. Dotted vessels were observed in all reports; however, the linear, pearl-like distribution as seen in our case was similar to that described by Zalaudek et al . [4] On the other hand, convolution of these pearly lines forming a reticular appearance was compatible with the reticular pattern mentioned by Bugatti et al. [2] and with a net-like pattern described by Lacorrubba et al . [5] The translucent collarette scaling we encountered was also reported by Bugatti et al. [2] Dermatoscopic findings of CCA are being reported. Some of the described features overlap each other. However, in our opinion, CCA reveals a particular dermatoscopic pattern. The dotted vessels following a linear distribution form an overall reticular appearance. Therefore, we conclude that global dermatoscopic appearance of CCA is a reticular pattern and locally, the vascular structure is due to the dotted vessels in a linear pearl-like distribution, namely, pearl-like vessels. The translucent collarette scaling is an additional dermatoscopic clue. Thus, dermatoscopy is a valuable tool in the diagnosis of CCA. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08122f1.jpg] [dv08122f2.jpg] |
| |||||||||

{kind=link}
{kind=link}