 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
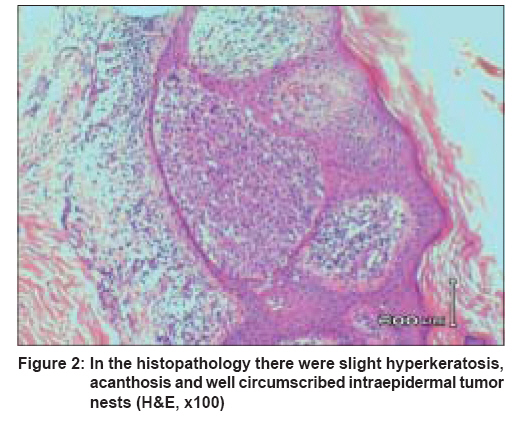
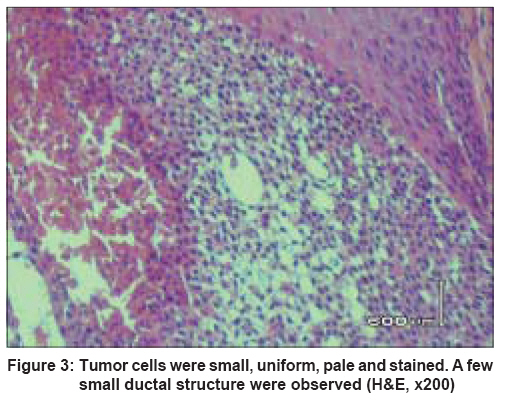
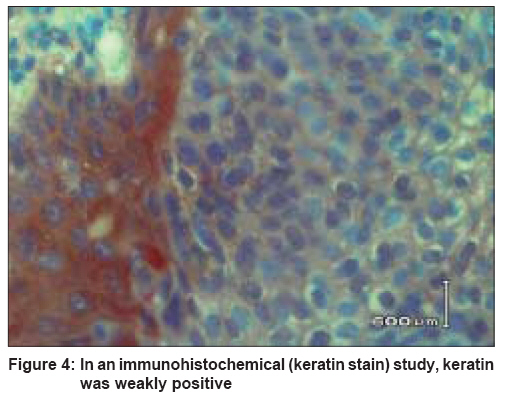
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 293-294 Quiz An annular, verrucous, and pruritic plaque on the back Ciralik Harun, Arican Ozer Department of Pathology, Medical Faculty, Kahramanmaras Sutcu Imam University, Kahramanmaras Code Number: dv08125 A 59-year-old white female with no previous health problem presented to our dermatology clinic with a lesion on the skin overlying the right scapula. It was asymptomatic, except for occasional pruritus. The size of the lesion had increased gradually from 3 mm to 30 mm over 25 years. At presentation, the lesion was a dry, annular, verrucous, brownish-pink, sharply demarcated plaque, measuring 2 x 3 cm [Figure - 1]. Histological examination of punch biopsy (3 mm) specimen, after hematoxylin and eosin staining [Figure - 2],[Figure - 3], and immunohistochemistry [Figure - 4] were done to study the characteristics of the lesion. What is the Diagnosis ? Diagnosis: Hidroacanthoma simplex The biopsy specimen of the verrucous plaque showed slight hyperkeratosis, acanthosis, and well-circumscribed intraepidermal tumor nests [Figure - 2]. Tumor cells were small, monomorphous and pale stained. A few small ductal structures were also observed [Figure - 3]. On immunohistochemistry, keratin was weakly positive [Figure - 4] and epithelial membrane antigen, S-100, and carcinoembryonic antigen were negative. The dermis was normal. Discussion Hidroacanthoma simplex (HAS) is a variant of poroma that is restricted to the epidermis. Poromas are benign neoplasms composed of poroid and cuticular cells. Four histopathologic variants of poromas are recognized, the categorization being according to the architectural features of the neoplasm: ( 1 ) eccrine poroma, which is a poroma connected to the epidermis and extending to the superficial dermis; ( 2 ) dermal duct tumor, in which the neoplasm is composed of small, solid aggregations of poroid and cuticular cells confined to the dermis, with little or no connection with the epidermis; ( 3 ) poroid hidradenoma, which is a solid-cystic, dermal poroma; and ( 4 ) hidroacanthoma simplex or intraepidermal poroma. [1] HAS, also termed intraepidermal poroma, was originally described by Smith and Coburn in 1956 as a single flat, elevated, or verrucous keratotic plaque resembling a flat type of seborrheic keratosis or a plaque of Bowen′s disease. Soon, other reports also appeared in the literature. [2] It is found mainly on the lower extremities and on the trunk in older persons, but the chest, arm, and face may be affected. It occurs at approximately equal frequency in males and females. [3],[4] Clinically, the lesion appears as a sharply demarcated, brownish, flat or verrucous plaque. [5] Histologically, HAS consists of discrete nests of cells confined to the epidermis. It may be confused with the clonal variant of seborrheic keratosis, basal cell epithelioma, or Bowen′s disease. [5] Based on the evidence from histopathological and ultrastructural studies, the neoplastic cells in HAS are thought to be the outer cells of the intraepidermal eccrine duct (external cells of the acrosyringium). [2] A histopathologic diagnosis of HAS can be made with certainty if the pathology sections show the following changes: typical intraepidermal, well-circumscribed nests composed of uniform basaloid, poroid cells within the acanthotic epidermis, and cystic or ductal structure in the nests. Without cystic or ductal structure, one might reasonably argue that many apparent case reports of HAS were not examples of HAS. Examples of malignant variants of HAS have been reported under different names, e.g., malignant HAS, in situ porocarcinoma, eccrine porocarcinoma, and HAS with invasive growth. [2] It is extremely rare for the diagnosis of HAS to be made clinically and, in most instances, the lesion is diagnosed as either Bowen′s disease or seborrheic keratosis. [3] Even if the lesion is diagnosed as benign HAS, it is always possible that malignant transformation may occur; alternatively, there may be coexistence of a malignant focus, with dermal invasion. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08125f4.jpg] [dv08125f3.jpg] [dv08125f2.jpg] [dv08125f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}