 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
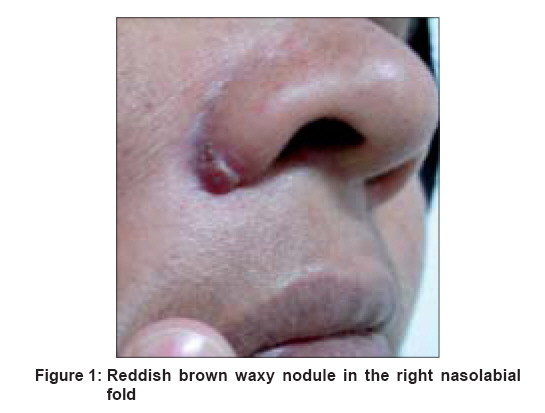
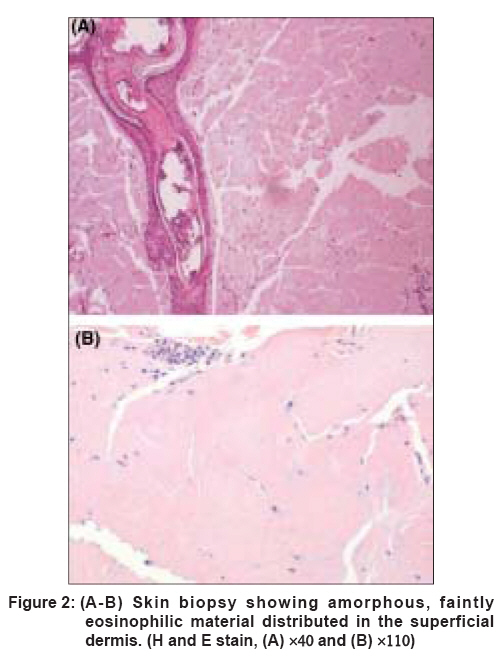
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 3, May-June, 2008, pp. 299 Net Quiz Nodule in the nasolabial fold Narang Tarun, Dogra Sunil, Handa Sanjeev, Radotra BishanDass Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh Code Number: dv08133 A 40-year-old female presented with spontaneous onset of a progressively enlarging nodule on the right side of her nose since 6 months. There was no history of itching, ulceration, or bleeding. She had been applying clobetasol propionate 0.05% ointment twice a day for the last 3 weeks but the lesions did not regress. Examination revealed a red-brown waxy nodule in the right nasolabial fold [Figure - 1]. No regional lymph nodes were palpable. There was no lesion on any other part of her body. She did not have any systemic complaints or any significant medical illness in the past. The lesion was completely excised and sent for histopathology. The biopsy revealed abundant deposits of amorphous, faintly eosinophilic hyaline material distributed in the perivascular and periadnexal tissues in the superficial dermis [Figure 2A] and [Figure 2B]. The material stained with special stains. What is the Diagnosis ? Diagnosis: Primary cutaneous nodular amyloidosis Results of the following laboratory tests were normal: complete blood cell counts, liver and renal biochemical parameters, serum calcium, phosphorus and chest x-ray. Serum IgA, IgG, and IgM levels were normal. Serum protein electrophoresis showed a minimal increase in gamma globulins. Serum and urine immunoelectrophoresis detected no monoclonal protein. No urinary Bence Jones proteins were detected. Discussion Amyloid deposits may be found in the skin with or without associated systemic disease. Primary localized cutaneous amyloidosis (PLCA) designates amyloidosis in the absence of systemic involvement and is of three types: lichen, macular, and nodular. Primary cutaneous nodular amyloidosis is the rarest form of PCLA. [1] Cutaneous lesions of nodular PLCA may be single or multiple. They consist of firm, smooth-surfaced, waxy or rubbery, pink to tan papules, plaques, or nodules measuring up to several centimeters. Clinically the lesions may be indistinguishable from nodular deposits of amyloid occurring in primary systemic amyloidosis or myeloma-associated amyloidosis. [2] Affected sites in nodular PLCA, in decreasing order of frequency are legs, head, trunk, arms, and genitalia. [3] The protein type deposited in nodular amyloid is of the AL type. Immunohistochemical studies of the dermal protein have revealed that the deposited protein can be light chains: lambda, kappa, or both. Gene-rearrangement studies have indicated that there is a clonal population of plasma cells producing amyloid protein in the skin; however, a similar clone has not been demonstrated in the bone marrow. [4] Patients diagnosed with primary cutaneous nodular amyloidosis need to be monitored for progression to systemic amyloidosis and plasma cell dyscrasias. Although previous studies have indicated the progression rate to be 50%, more recent studies have demonstrated a much lower rate of 7%. [5] The majority of these patients do well and remain in good general health. Secondary cutaneous amyloidosis may be found in association with benign and malignant cutaneous neoplasms. The amyloid in these skin lesions is AK-type. It is usually found in association with basal cell carcinomas and, much more rarely, in squamous cell carcinoma, adnexal tumors, and seborrheic and actinic keratosis. The key histological feature of nodular cutaneous amyloidosis is the presence of hyaline, eosinophilic masses filling the entire dermis. [2] Unlike lichen and macular amyloidosis where protein is deposited into the papillary dermis alone, nodular amyloidosis affects the dermis, subcutis, and blood vessels. [1],[2] Amyloid stains with Congo red, Sirius red, thioflavin T, methyl violet, crystal violet, and periodic acid-Schiff, although no single stain is both highly sensitive and specific. Electron microscopy reveals amyloid deposits composed of randomly arranged, straight, nonbranching filaments measuring 6-10 nm in diameter. Treatment of nodular cutaneous amyloidosis is by local destruction to improve appearance. Treatment options for nodular amyloidosis include surgical excision, cryotherapy, electrodessication cautery, and carbon dioxide and pulsed dye laser. [5],[6],[7] Notably, nodular amyloidosis exhibits a high recurrence rate, often requiring multiple treatments. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08133f1.jpg] [dv08133f2.jpg] |
| |||||||||

{kind=link}
{kind=link}