
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 7, 2008, pp. 5-12
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 7, Supp. 1, January, , 2008, pp. 5-12
Recommendations
Standard guidelines of care for chemical peels
Khunger Niti
Member, IADVL Task Force*, Department of Dermatology, Safdarjung Hospital, New Delhi
Correspondence Address:Department of Dermatology, Safdarjung Hospital, New Delhi
drniti@rediffmail.com
Code Number: dv08136
Abstract Chemical peeling is the application of a chemical agent to the skin, which causes controlled destruction of a part of or the entire epidermis, with or without the dermis, leading to exfoliation and removal of superficial lesions, followed by regeneration of new epidermal and dermal tissues.
Indications for chemical peeling include pigmentary disorders, superficial acne scars, ageing skin changes, and benign epidermal growths.
Contraindications include patients with active bacterial, viral or fungal infection, tendency to keloid formation, facial dermatitis, taking photosensitizing medications and unrealistic expectations.
Physicians' qualifications : The physician performing chemical peeling should have completed postgraduate training in dermatology. The training for chemical peeling may be acquired during post graduation or later at a center that provides education and training in cutaneous surgery or in focused workshops providing such training. The physician should have adequate knowledge of the different peeling agents used, the process of wound healing, the technique as well as the identification and management of complications.
Facility : Chemical peeling can be performed safely in any clinic/outpatient day care dermatosurgical facility.
Preoperative counseling and Informed consent : A detailed consent form listing details about the procedure and possible complications should be signed by the patient. The consent form should specifically state the limitations of the procedure and should clearly mention if more procedures are needed for proper results. The patient should be provided with adequate opportunity to seek information through brochures, presentations, and personal discussions. The need for postoperative medical therapy should be emphasized.
Superficial peels are considered safe in Indian patients.
Medium depth peels should be performed with great caution, especially in dark skinned patients.
Deep peels are not recommended for Indian skin. It is essential to do prepeel priming of the patient's skin with sunscreens, hydroquinone and tretinoin for 2-4 weeks.
Endpoints in peels: For glycolic acid peels: The peel is neutralized after a predetermined duration of time (usually three minutes). However, if erythema or epidermolysis occurs, seen as grayish white appearance of the epidermis or as small blisters, the peel must be immediately neutralized with 10-15% sodium bicarbonate solution, regardless of the duration of application of the peel. The end-point is frosting for TCA peels, which are neutralized either with a neutralizing agent or cold water, starting from the eyelids and then the entire face. For salicylic acid peels, the end point is the pseudofrost formed when the salicylic acid crystallizes. Generally, 1-3 coats are applied to get an even frost; it is then washed with water after 3-5 minutes, after the burning has subsided. Jessner's solution is applied in 1-3 coats until even frosting is achieved or erythema is seen. Postoperative care includes sunscreens and moisturizers Peels may be repeated weekly, fortnightly or monthly, depending on the type and depth of the peel.
Keywords: Glycolic acid, Trichloroacetic acid, Salicylic acid
Introduction
The concept of peeling the skin to improve the texture, smoothen and beautify it has been used since ancient times. In ancient Egypt, Cleopatra used sour milk, now known to contain lactic acid, an alpha hydroxy acid while French women used old wine containing tartaric acid, to enhance the appearance of the skin. [1],[2] Chemical peeling is a common office procedure that has evolved over the years, using the scientific knowledge of wound healing after controlled chemical skin injury. [3] In spite of the advent of newer techniques and lasers, peeling has stood the test of time as a simple procedure, requiring hardly any instrumentation to rejuvenate the skin.
Definition
Chemical peeling is the application of a chemical agent to the skin, which causes controlled destruction of a part or entire epidermis, with or without the dermis, leading to exfoliation, removal of superficial lesions, followed by regeneration of new epidermal and dermal tissues.
Rationale and Scope These guidelines identify the indications for chemical peels, various agents that can be utilized, methodology, pre- and postpeel care, associated complications, and expected results.
Indications of Chemical Peels[1],[4]
Pigmentary disorders
- Melasma
- Postinflammatory hyperpigmentation
- Freckles
- Lentigines
- Facial melanoses
Acne
- Superficial acne scars
- Postacne pigmentation
- Comedonal acne
- Acne excoriιe
- Acne vulgaris-mild to moderately severe acne
Aesthetic
- Photoaging
- Fine superficial wrinkling
- Dilated pores
- Superficial scars
Epidermal growths
- Seborrheic keratoses
- Actinic keratoses
- Warts
- Milia
- Sebaceous hyperplasia
- Dermatoses papulosa nigra
Contraindications[1],[4]
- Active bacterial, viral, fungal or herpetic infection
- Open wounds
- H/O (history of) drugs with photosensitizing potential
- Preexisting inflammatory dermatoses such as psoriasis, atopic dermatitis
- Uncooperative patient (patient is careless about sun exposure or application of medicine)
- Patient with unrealistic expectations.
- For medium depth and deep peels-history of abnormal scarring, keloids, atrophic skin, and isotretinoin use in the last six months. [5]
Physicians′ Qualifications
1. General
- The physician should be a trained dermatologist.
- The physician should have knowledge of the skin and subcutaneous tissue, including structural and functional differences and variations in skin anatomy of the facial cosmetic unit.
2. Specific
- The physician should have appropriate training in chemical peeling either during postgraduation or later at a center that routinely provides education and training in cutaneous surgery. Such training may also be obtained in focused workshops providing such training.
- The physician should have knowledge of the basic chemistry of peels, such as acids, bases, pH and pK a of peeling solutions and the mechanism of action of peels. [5] Familiarity with the properties of each peeling agent to be used is critical for successful outcome.
- The physician should know all aspects of mechanism of wound healing after chemical skin injury.
- The physician should be well versed with all aspects of pathogenesis and the medical therapy of the condition to be peeled, such as melasma, acne, photodamage etc.
- The physician should be well versed with early recognition, prevention and treatment of postoperative complications such as prolonged erythema, postinflammatory hyperpigmentation, impending scarring etc.
Prepeel Assessment
A. History should include general medical history, degree of sun exposure, occupation to judge the level of sun exposure, history of herpes simplex, recent isotretinoin treatment in the last six months (for medium depth and deep peels), keloidal tendency, tendency for postinflammatory hyperpigmentation, current medications, any previous surgical treatment, immunocompromising conditions, and smoking (may delay healing in deep peels; this is not relevant for superficial peels). In patients in whom phenol peels are planned, history of systemic disease, particularly cardiac disease, should be taken.
B. Detailed medical examination should include general physical and cutaneous examination including skin type, degree of photoaging, degree of sebaceous activity (oily or dry skin), presence of postinflammatory hyperpigmentation, keloid or hypertrophic scar, infection, and preexisting inflammation.
C. Investigations
- Skin biopsy should be done when indicated, to confirm diagnoses and see the level of pigmentation, e.g ., mixed or dermal melasma, lichen planus pigmentosus. No specific investigations are indicated for superficial peels.
- In patients in whom deep (phenol) peels are planned, hemogram, urinalysis, liver and renal function tests and electrocardiograph may be carried out as cardiac complications such as life-threatening arrhythmia, are recognized as complications of deep peeling.
D. Documentation
- Informed consent after counseling as below
- Photographic record
Counseling: Proper counseling is very important and should include:
- Evaluation of the psychological aspects to judge the motivation and expectations of the patient.
- Explanation that patient should have realistic expectations; this is particularly important in the media-hyped patient who may have unrealistic expectations.
- Explanation about the nature of treatment, expected outcome. It is advisable to downplay the degree of improvement expected.
- Information about the time taken for recovery of normal skin and importance of maintenance regimens.
- Discussion of side effects, likely and unlikely complications, and particularly, pigmentation changes.
Preprocedure treatment recommendations (Priming): [1],[5],[6] Priming is essential for at least 2-4 weeks prior to the procedure. Priming helps to reduce wound healing time, facilitates uniform penetration of peeling agent, detects intolerance to any agent, enforces patient compliance and reduces the risk of complications.
- Control any active infection or preexisting dermatoses.
- Broad-spectrum sunscreens.
- Hydroquinone (2-4%) in patients prone to postinflammatory hyperpigmentation.
- Patients may also be primed at home by using mild topical peeling agents such as tretinoin 0.025%, adapalene 0.1%, Glycolic acid 6-12%, kojic acid, azelaic acid, etc (agents which are likely to be used in postprocedure maintenance). Tretinoin is known to reduce healing time after resurfacing. [7] The choice of the priming agent depends on the individual physician′s preference and individualized patient requirements.
- In patients with history of herpes simplex posted for medium depth and deep peels, antiviral therapy with acyclovir or famciclovir is recommended, beginning two days prior to the procedure and continued for 7-10 days until complete reepithelialization.
Reagents
- Correctly labeled peeling agents in various concentrations
- Alcohol to clean the skin
- Acetone to degrease the skin
- Cold water
- Syringes filled with normal saline for irrigation of the eyes, in case of accidental spillage.
- Neutralizing solutions: Specific neutralizers are mentioned under "description of individual peels."
Equipment
- Glass cup or beaker in which the required agent is poured
- Head band or cap for the patient
- Gloves
- Cotton-tipped applicators or swab sticks
- 2" x 2" cotton gauze pieces
- Fan for cooling
- Timer for alpha-hydroxy acid peels
Peeling Agents
- Alpha-hydroxy acids, AHA Monocarboxylic acids: Glycolic acid (Level A) [8],[9],[10],[11],[12],[13],[14] , Lactic acid [15] (Level B), Bicarboxylic acid: Malic acid (Level C), Tricarboxylic acid: Citric acid (Level C)
- Beta-hydroxy acids, BHA (salicylic acid) [16],[17],[18],[19] (Level A)
- Trichloroacetic acid (TCA) [20],[21],[22] (Level A)
- Alpha-keto acids (pyruvic acid) [23] (Level C)
- Resorcinol (Level B)
- Jessners solution [24],[ 25] (Salicylic acid 14 g, Lactic acid 14 g, Resorcinol 14 g with Ethanol to make 100 mL) (Level B)
- Retinoic acid [26] (Level C)
- Phenol [27],[28],[29],[30] Type I-II skin (Level A) Type III-IV skin (Level C)
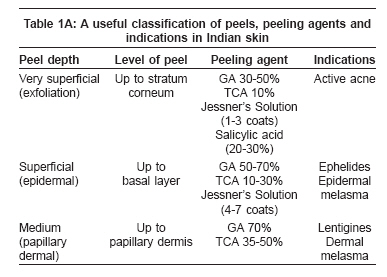
Classification of peels according to the histological depth of necrosis: [5]
A. Very Superficial light peels : Necrosis up to the level of stratum corneum. Agents used: TCA 10%, GA 30-50%, Salicylic acid 20-30%, Jessner′s solution 1-3 coats, Tretinoin 1-5%
B. Superficial light peels : Necrosis through the entire epidermis up to basal layer. Agents used: TCA 10-30%, GA 50-70%, Jessner′s solution 4-7 coats
C. Medium depth peels : Necrosis up to upper reticular dermis. Agents used: TCA 35-50%, GA 70% plus TCA 35%, 88% phenol un-occluded, Jessner′s solution plus TCA 35%, solid CO 2 plus TCA 35%
D. Deep peels : Necrosis up to mid-reticular dermis. Agents used: Baker-Gordon phenol peel
Recommendations
Anesthesia: Anesthesia is not required in superficial and medium depth peels. Mild tranquilizers or anxiolytics may be used in anxious patients.
Safety Precautions before peeling : The label on the bottle must be checked before applying the peel; the head should be elevated to 45° . To avoid accidental spillage, the open bottle or the soaked applicator should not be passed over the face. A syringe filled with water or saline should be kept ready for irrigation of the eyes in case of accidental spillage.
Skin preparation before peeling
- The patient is asked to wash the face with soap and water.
- The hair is pulled back with a hair band or cap.
- The patient lies down with head elevated to 45° with the eyes closed.
- Using 2" x 2" gauze pieces, the skin is cleaned with alcohol and then degreased with acetone.
Procedure for Superficial Peels[1],[4],[8]
- The required strength of the peeling agent is poured into a glass beaker and the neutralizing agent is also kept ready.
- Sensitive areas like the inner canthus of the eyes and nasolabial folds are protected with Vaseline.
- The peeling agent is then applied either with a brush or cotton-tipped applicator or gauze.
- The chemical is applied quickly as cosmetic units on the entire face, beginning from the forehead, then the right cheek, nose, left cheek and chin in that order. If required, the perioral, upper and lower eyelids are treated last. Feathering strokes are applied at the edges to blend with surrounding skin and prevent demarcation lines.
- For glycolic acid peels, the peel is neutralized after the predetermined duration of time (usually three minutes). However, if erythema or epidermolysis occurs, seen as grayish white appearance of the epidermis or small blisters, the peel must be neutralized immediately irrespective of the duration. Neutralization is done with 10-15% sodium bicarbonate solution or neutralizing lotion and then, washed off with water.
- For TCA peels, the end-point is frosting and neutralization is either with a neutralizing agent or cold water, starting from the eyelids and then the entire face.
- When the salicylic acid peel is applied, it crystallizes forming a pseudo-frost; generally, 1-3 coats are applied to get an even frost. It is then washed with water after 3-5 minutes, after the burning subsides.
- Jessner′s solution is applied in 1-3 coats to get even frosting; the endpoint is erythema or even frosting.
- A cooling fan helps to reduce burning of the skin.
- The skin is gently dried with gauze and the patient is asked to wash with cold water until the burning subsides. The face is patted dry; rubbing should be avoided.
- Tretinoin peels are yellow peels that are left on for 4-5 hours and then washed away.
- Very superficial peels may be repeated every 1-2 weeks and superficial peels every 2-4 weeks.
Medium Depth and Deep Peels Medium depth peels should be done with great caution in dark skinned patients because of the high risk of prolonged hyperpigmentation. [1],[31] Deep phenol peels are not recommended for dark skins of types IV-VI because of high risk of prolonged or permanent pigmentary changes, [1] although modified phenol peels are being used in types III-IV Asian skins. [28],[29],[30]
Postoperative Care The aim of good postoperative care is to prevent or minimize complications and ensure early recovery. This is most important in dark skinned patients in whom pigmentary alterations are common. A careful maintenance program is essential to maintain the results of chemical peeling in most patients.
- In the postpeel period, edema, erythema and desquamation occur. In superficial peels, this lasts for 1-3 days, whereas in deeper peels, it lasts for 5-10 days.
- Mild soap or a non-soap cleanser may be used. If there is crusting, a topical antibacterial ointment should be used to prevent bacterial infection.
- Clear instructions must be given to the patient for the postprocedure period.
- Cold compresses or calamine lotion may be used to soothe the skin.
- They should be told to use broad-spectrum sunscreens and only bland moisturizers until peeling is complete.
- They should avoid peeling or scratching the skin.
- Analgesics are not usually needed but may be advised in case of burning sensation.
Complications[1],[32],[33],[34],[35]
Proper patient selection, adequate counseling, priming the skin and supportive medical therapy in addition to good intra- and postoperative care, are essential for satisfactory cosmetic results. The best way to avoid complications is to identify patients at risk and use lighter peels. The deeper the peel, the greater is the risk of complications. The patients at risk are those with a history of postinflammatory hyperpigmentation, keloid formation, heavy occupational exposure to sun such as field workers, uncooperative patients and patients with a history of sensitive skin who are unable to tolerate sunscreens, hydroquinone etc.
- Pigmentary changes: Postinflammatory hyperpigmentation and hypopigmentation. These can be very persistent and often difficult to treat. They may be treated with broad-spectrum sunscreens, topical corticosteroids, tretinoin, hydroquinone or alpha-hydroxy acids.
- Infection: Bacterial ( Staphylococcus , Streptococcus , Pseudomonas ), viral (Herpes simplex) and fungal (Candida). They should be treated aggressively and appropriately.
- Scarring is rare in superficial peels. Proper priming, proper choice of peeling agent and postoperative care can help in prevention of this complication.
- Allergic reactions
- Milia
- Acneiform eruptions
- Lines of demarcation
- Textural changes
- Persistent erythema: Erythema persisting for more than three weeks after a peel, is indicative of early scarring and should be treated with potent topical corticosteroids for £ 2 weeks.
- Toxicity: Although rare, it may occur with resorcinol, salicylic acid and phenol. [5]
Combination Peels and Procedures A. combination of peeling agents enhances the depth of the peel without using a higher concentration of the peeling agent. However, these medium depth peels should be used cautiously in darker skinned patients because of the risk of uneven depth of peeling and increased risk of side effects, such as postinflammatory hyperpigmentation and scarring.
- Glycolic acid 70% combined with TCA 35% (Coleman′s Peel) [36] (level C). In darker skins, lower concentrations of TCA (10-25%) may be used (level D). [1]
- Solid CO 2 combined with 35% TCA (Brody′s peel) (level C).
- Jessner′s solution with 35% TCA (Monheit′s Peel) (level C). [37]
B. Two procedures can also be combined to blend cosmetic units and avoid demarcation lines: [38],[39],[40]
- Chemical peeling combined with dermabrasion: This procedure was originally used by combining application of 50% TCA followed by dermabrasion for post-acne scarring. However, 50% TCA causes scarring and its use is not advocated anymore.
- Chemical peeling can also be combined with laser resurfacing for skin rejuvenation. First, a chemical peel is performed and then, the deeper wrinkles in the periorbital and perioral areas are treated with pulsed CO 2 laser (level C).
- Chemical Peel with dermasanding using sandpaper (level C).
- Chemical peeling with Botulinum Toxin (level C).
- Chemical peeling with fillers (level C).
Conclusions
Chemical peeling is a simple office procedure used for the treatment of dyschromias, photoaging, and superficial scarring that can lead to excellent cosmetic improvement, when repeatedly performed in carefully selected patients. Although various depths of peels have been described, superficial and medium depth peels are safer for Indian patients. Deep chemical peels should be avoided because of the risk of permanent pigmentary changes. The type, depth and concentration of the peel should be selected according to the pathology of the condition [Table - 1a & 1b]. Chemical peels are not one-time procedures and should be repeated with maintenance peels to achieve maximum improvement and prevent recurrence. With the advent of lasers and newer techniques, the use of chemical peels has declined; however, its simplicity as an office procedure, minimal morbidity, easy availability and cost-effectiveness ensure that it still holds an important place as a tool to treat dyschromias and photoaging. Careful patient selection, priming of the skin, standardization of peels, postpeel care and maintenance programs are essential to achieve excellent cosmetic results.
References
| 1. | Savant SS. Superficial and medium depth chemical peeling. In: Text book of dermatosurgery and cosmetology. In: Savant SS, editor. 2 nd ed. ASCAD; 2005. p. 177-95 Back to cited text no. 1 |
| 2. | Brody H. History of chemical peels. In: Baxter S, editor. Chemical peeling and resurfacing. 2nd ed. St. Louis: Mosby Year Book Inc; 1997. p. 1-5. Back to cited text no. 2 |
| 3. | Stegman SJ. A comparative histologic study of the effects of the three peeling agents and dermabrasion on normal and sun damaged skin. Aesth Plast Surg 1982;6:123-35. Back to cited text no. 3 |
| 4. | Monheit GD, Kayal JD. Chemical peeling. In Techniques of Dermatologic Surgery. Nouri K, Leal-Khouri, editors. Elsevier; 2003. p. 233-44. Back to cited text no. 4 |
| 5. | Chemical Peels. In: Rubin MG, editor. Procedures in cosmetic dermatology. Elsevier Inc.; 2006 p. 1-12. Back to cited text no. 5 |
| 6. | Roenigk RK, Retinoids, dermabrasion, chemical peel and keloids. In: Roenigk RK, Roenigk HH Jr, editors. Surgical Dermatology: advances in current practice. St Louis: Mosby; 1993. p. 376-83. Back to cited text no. 6 |
| 7. | Hevia O, Nemeth AJ, Taylor JR. Tretinoin accelerates healing after TCA chemical peels. Arch Dermatol 1991;127:678-82. Back to cited text no. 7 [PUBMED] |
| 8. | Rubin MG. Glycolic acid peels. Manual of chemical peels-superfical and medium depth. In: Rubin MG, editor, 1st ed. Philadelphia: JB Lippincot Co; 1995. p. 89-102. Back to cited text no. 8 |
| 9. | Ditre CM. Alpha-hydroxy acid peels. Chemical Peels. Procedures in cosmetic dermatology. In: Rubin MG, editor. Elsevier Inc.; 2006. p. 27-40. Back to cited text no. 9 |
| 10. | Grover C, Reddy BS. The therapeutic value of glycolic acid peels in dermatology. Indian J Dermatol Venereol Leprol 2003;69:148-50. Back to cited text no. 10 |
| 11. | Javaheri SM, Handa S, Kaur I, Kumar B. Safety and efficacy of glycolic acid facial peel in Indian women with melasma. Int J Dermatol 2001;40:354-7. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Wang CM, Huang CL, Hu CT, Chan HL. The effect of glycolic acid on treatment of acne in Asian skin. Dermatol Surg 1997;23:23-9. Back to cited text no. 12 [PUBMED] |
| 13. | Lim JTE, Tham SN. Glycolic acid peels in the treatment of melasma among Asian women. Dermatol Surg 1997;23:177-9. Back to cited text no. 13 |
| 14. | Burns RL, Prevost-Blank PL, Lawry MA, Lawry TB, Faria DT, Fivenson DP. Glycolic acid for post inflammatory hyperpigmentation in black patients. Dermatol Surg 1997;23:171-5. Back to cited text no. 14 [PUBMED] |
| 15. | Sharquie KE, Al-Tikreety MM, Al-Mashhadani SA. Lactic acid as a new therapeutic peeling agent in melasma. Dermatol Surg 2005;31:149-54. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Vedamurthy M. Salicylic acid peels. Indian J Dermatol Venereol Leprol 2004;70:136-8. Back to cited text no. 16 |
| 17. | Lee HS, Kim IH. Salicylic acid peels for the treatment of acne vulgaris in Asian patients. Dermatol Surg 2003;5:1196-9. Back to cited text no. 17 |
| 18. | Grimes PE. Salicylic acid peels. Chemical Peels. Procedures in cosmetic dermatology. In: Rubin MG, editor. Elsevier Inc.; 2006. p. 47-55. Back to cited text no. 18 |
| 19. | Bari AU, Iqbal Z, Rahman SB. Tolerance and safety of superficial chemical peeling with salicylic acid in various facial dermatoses. Indian J Dermatol Venereol Leprol 2005;71:87-90. Back to cited text no. 19 [PUBMED] [FULLTEXT] |
| 20. | Leonhardt JM, Lawrence N. Trichloroacetic acid (TCA) peels. Chemical Peels. Procedures in cosmetic dermatology. In: Rubin MG, editor. Elsevier Inc.; 2006. p. 73-86. Back to cited text no. 20 |
| 21. | Chun EY, Lee JB, Lee KH. Focal trichloracetic acid peel method for benign pigmented lesions in dark-skinned patients. Dermatol Surg 2004;30:512-6. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
| 22. | Rubin MG. Trichloroacetic acid peels. Manual of chemical peels-superfical and medium depth. In: Rubin MG, editor, 1st ed. Philadelphia: JB Lippincot Co.; 1995. p. 110-29. Back to cited text no. 22 |
| 23. | Ghersetich I, Brazzini B, Peris K, Cotellessa C, Manunta T, Lotti T. Pyruvic acid peels for the treatment of photoaging. Dermatol Surg 2004;30:32-6. Back to cited text no. 23 [PUBMED] [FULLTEXT] |
| 24. | Rubin MG. Jessner's peels. Manual of chemical peels-superfical and medium depth. In: Rubin MG, editor, 1 st ed. Philadelphia: JB Lippincot Co.; 1995. p. 79-88. Back to cited text no. 24 |
| 25. | Fulton JE Jr. Jessner's Peel. Chemical Peels. Procedures in cosmetic dermatology. In: Rubin MG, editor, Elsevier Inc. 2006. p. 57-71. Back to cited text no. 25 |
| 26. | Khunger N, Sarkar R, Jain RK. Tretinoin peels versus glycolic acid peels in the treatment of Melasma in dark-skinned patients. Dermatol Surg 2004;30:756-60. Back to cited text no. 26 [PUBMED] [FULLTEXT] |
| 27. | Stone PA. Phenol peeling. Chemical Peels. Procedures in cosmetic dermatology. In: Rubin MG, editor, Elsevier Inc.; 2006. p. 87-114. Back to cited text no. 27 |
| 28. | Piamphongsant T. Phenol-castor oil: Modified peel for dermal melasma. Dermatol Surg 2006;32:611-7. Back to cited text no. 28 [PUBMED] [FULLTEXT] |
| 29. | Park JH, Choi YD, Kim SW, Kim YC, Park SW. Effectiveness of modified phenol peel (Exoderm) on facial wrinkles, acne scars and other skin problems of Asian patients. J Dermatol 2007;34:17-24. Back to cited text no. 29 [PUBMED] [FULLTEXT] |
| 30. | Landau M. Cardiac complications in deep chemical peels. Dermatol Surg 2007;33:190-3. Back to cited text no. 30 [PUBMED] [FULLTEXT] |
| 31. | Al-Waiz MM, Al-Sharqi AI. Medium-depth chemical peels in the treatment of acne scars in dark-skinned individuals. Dermatol Surg 2002;28:383-7. Back to cited text no. 31 [PUBMED] [FULLTEXT] |
| 32. | Resnick SS, Resnick BI. Complications of chemical peeling. Dermatol Clin 1995;13:309-12. Back to cited text no. 32 |
| 33. | Duffy DM. Avoiding complications. Chemical Peels. Procedures in cosmetic dermatology. In: Rubin MG, editor, Elsevier Inc.; 2006. p. 137-69. Back to cited text no. 33 |
| 34. | Baumann L. Chemical Peeling. Cosmetic dermatology. Principles and Practice. In: Baumannn L, editor. 1 st ed, New York: The McGraw- Hill Companies; 2002. p. 173-86. Back to cited text no. 34 |
| 35. | Moy LS. Superficial chemical peels with alpha-hydroxy acids. Atlas of cutaneous surgery. In: Robinson JK, Arndt KA, Le Boit PE, Wintroub BU, editors. Philadelphia: WB Saunders Company; 1996. p. 345-350. Back to cited text no. 35 |
| 36. | Coleman WP 3rd, Futrell JM. The glycolic, trichloroacetic acid peel. J Dermatol Surg Oncol 1994;20:76-80. Back to cited text no. 36 [PUBMED] |
| 37. | Monheit GD. The Jessner's + TCA peel: A medium-depth chemical peel. J Dermatol Surg Oncol 1989;15:953-63. Back to cited text no. 37 |
| 38. | Monheit GD. Combinations of therapy. Chemical peels. In: Rubin MG, editor, Chemical Peels. Procedures in cosmetic dermatology. Elsevier Inc.; 2006. p. 115-36. Back to cited text no. 38 |
| 39. | Fulton JE, Rahimi D, Helton P, Dahlberg K. Neck rejuvenation by combining Jessner/TCA peel, dermasanding and CO2 laser resurfacing. Dermatol Surg 1999;25:745-50. Back to cited text no. 39 |
| 40. | Landau M. Combination of chemical peelings with botulinum toxin injections and dermal fillers. J Cosmet Dermatol 2006;5:121-6. Back to cited text no. 40 [PUBMED] |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08136t1b.jpg]
[dv08136t1a.jpg]
|

{kind=link}
{kind=link}