 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
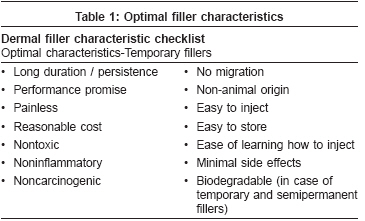
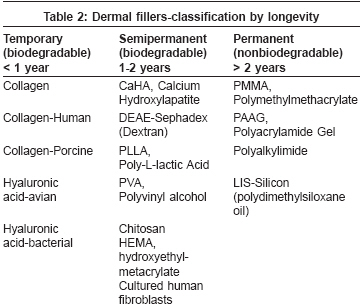
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 7, Supp. 1, January, , 2008, pp. 23-27 Recommendations Standard guidelines for the use of dermal fillers Vedamurthy Maya Member, IADVL Dermatosurgery Task Force* and Consultant Dermatologist, Apollo Hospitals, Chennai Code Number: dv08138 Abstract Currently used fillers vary greatly in their sources, efficacy duration and site of deposition; detailed knowledge of these properties is essential for administering them. Indications for fillers include facial lines (wrinkles, folds), lip enhancement, facial deformities, depressed scars, periocular melanoses, sunken eyes, dermatological diseases-angular cheilitis, scleroderma, AIDS lipoatrophy, earlobe plumping, earring ptosis, hand, neck, dιcolletι rejuvenation.Physicians' qualifications : Any qualified dermatologist may use fillers after receiving adequate training in the field. This may be obtained either during postgraduation or at any workshop dedicated to the subject of fillers. The physicians should have a thorough knowledge of the anatomy of the area designated to receive an injection of fillers and the aesthetic principles involved. They should also have a thorough knowledge of the chemical nature of the material of the filler, its longevity, injection techniques, and any possible side effects. Facility: Fillers can be administered in the dermatologist's minor procedure room. Preoperative counseling and informed consent: Detailed counseling with respect to the treatment, desired effects, and longevity of the filler should be discussed with the patient. Patients should be given brochures to study and adequate opportunity to seek information. Detailed consent forms need to be completed by the patients. A consent form should include the type of filler, longevity expected and possible postoperative complications. Preoperative photography should be carried out. Choice of the filler depends on the site, type of defect, results needed, and the physician's experience. Injection technique and volume depend on the filler and the physician's preference, as outlined in these guidelines. Keywords: Wrinkles, Static wrinkles, Aging, Scars, Fillers Introduction[1],[2] Dermal fillers are substances used in soft tissue augmentation to enhance or replace volume that is lost in any part of the skin or subcutaneous fat. Fillers form an effective tool in rejuvenation, either as a stand-alone treatment or in combination with other procedures such as Laser resurfacing or botulinum toxin. [1] The use of dermal fillers in soft tissue augmentation is undergoing a renaissance period with many new filler materials appearing in the market. The practice of soft tissue augmentation was started by Neuber in 1893, who took fat from the arms and transplanted it into facial defects. In 1899, paraffin was used and was later given up due to foreign body granulomasor paraffinomas. In the 1940s and 1950s, silicone was used extensively until the commissioner of the US-Food and Drug Administration (US-FDA) declared the use of injectable silicone to be illegal. The field of softtissue augmentation underwent a revolutionary change in the early 1970s when researchersat Stanford University worked on the use of animal and human collagen as implant materials. The search for an ideal, permanent dermal filler is still ongoing and no single,currently available filler meets all expectations of the physician. Rationale and Scope With an increasing number of filler materials flooding the market place, any physician practicing soft tissue augmentation should possess a thorough knowledge of the filler material, including the mode of action of every material, its technique of injection, its limitations, advantages and disadvantages. These guidelines provide a minimal framework for reference to the practicing dermatologist. The field of fillers is a rapidly evolving one, with new fillers being introduced every year but no controlled, long-term data for long-term efficacy and longevity. These guidelines are therefore based on available data and experience of the task force members.Dermal Fillers-Materials, Characters, Types and Classification Dermal filler products possess a number of attributes: substances, substance source, compounds, performance, duration and mechanism of action, consistency, approved indication(s), and substantiation. Preferences of patients and providers may differ. With temporary fillers, per injection costs are less and complications are minor and rare. However, long-term maintenance costs are higher due to the necessity of repeated injections. With longer-duration fillers, the time-and-cost horizon is shortened but any complication can potentially be more significant. A balance is achieved when all factors are taken into consideration and tempered by the provider′s expertise and the patient′s expectations and acceptance of potential outcomes. While the perfect filler is yet to be available, characteristics of optimal filler are listed in [Table - 1].Types of Fillers[3],[4],[5] Fillers can be classified based on different criteria: 1) Based on longevity: Fillers are classified as temporary, semipermanent, and permanent depending on the longevity of action, as shown in [Table - 2]. 2) Based on site of placement
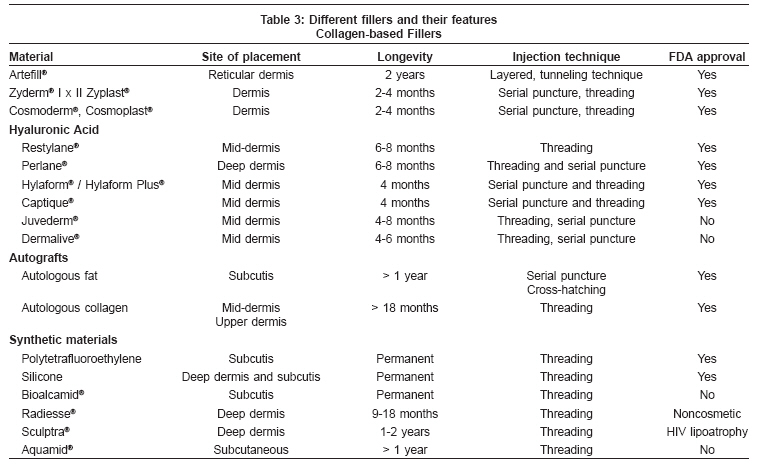
[Table - 3] summarizes different fillers, site of placement, injection technique and their approval status from FDA. Various brands are available in different parts of the world and it is therefore not possible to list every brand of filler available in the market. Annexure 1 shows different brands that are available. New fillers are introduced every year and it is therefore recommended that the physician seek full information from the manufacturer /distributor before using a filler. Task Force Recommendations: Level D
Indications: Level C[3]
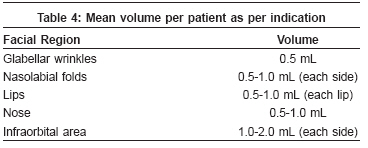
Of these, the most common indications of fillers are wrinkles, scars, lips, and lipoatrophy. Informed consent should be taken after proper counseling of the patient. The consent form should include full details about the filler (chemical nature and source) to be administered, indication for which the filler is being used, expected longevity of results, its approval status, possible side effects and the cost. Preoperative Preparation: Level C[6]
Intraoperative Procedure: Level C[6]
Postprocedural Precautions and Advice
Complications: Level C[7],[8],[9],[10] Complications are infrequentand usually minor; usually, permanent and long-term fillers have greater risk for complications. These include: Immediate complications
Conclusion In a short span of time, fillers have come to play an important role in the nonsurgical management of ageing skin. The technique is a safe, simple and effective modality, when used by a properly trained physician. Proper knowledge of the anatomy of the area of injection, aesthetic sense and proper patient selection are essential. Fillers can also be combined with other aesthetictreatments such as Botox, microdermabrasion, peels, thread-lifts, and Laser resurfacing. As in all aesthetic techniques, proper patient counseling with respect to achievable results is important.Acknowledgment The author is are indebted to Dr Apratim Goel for her inputs while preparing these guidelinesReferences
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08138t2.jpg] [dv08138t4.jpg] [dv08138t1.jpg] [dv08138t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}