 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 7, Supp. 1, January, , 2008, pp. 37-45 Recommendations Standard guidelines of care for vitiligo surgery Parsad Davinder, Gupta Somesh Members, IADVL Dermatosurgery Task Force*, Department of Dermatology, Postgraduate Institute of Medical Education & Research, Chandigarh Code Number: dv08140 Abstract Vitiligo surgery is an effective method of treatment for selected, resistant vitiligo patches in patients with vitiligo.Physician's qualifications: The physician performing vitiligo surgery should have completed postgraduate training in dermatology which included training in vitiligo surgery. If the center for postgraduation does not provide education and training in cutaneous surgery, the training may be obtained at the surgical table (hands-on) under the supervision of an appropriately trained and experienced dermatosurgeon at a center that routinely performs the procedure. Training may also be obtained in dedicated workshops. In addition to the surgical techniques, training should include local anesthesia and emergency resuscitation and care. Facility: Vitiligo surgery can be performed safely in an outpatient day care dermatosurgical facility. The day care theater should be equipped with facilities for monitoring and handling emergencies. A plan for handling emergencies should be in place, with which all nursing staff should be familiar. Vitiligo grafting for extensive areas may need general anesthesia and full operation theater facility in a hospital setting and the presence of an anesthetist is recommended in such cases. Indications for vitiligo surgery : Surgery is indicated for stable vitiligo that does not respond to medical treatment. While there is no consensus on definitive parameters for stability, the Task Force suggests the absence of progression of disease for the past one year as a definition of stability. Test grafting may be performed in doubtful cases to detect stability. Preoperative counseling and Informed consent: A detailed consent form elaborating the procedure and possible complications should be signed by the patient. The patient should be informed of the nature of the disease and that the determination of stability is only a vague guide. The consent form should specifically state the limitations of the procedure, about the possible future progression of disease and whether more procedures will be needed for proper results. The patient should be provided with adequate opportunity to seek information through brochures and one-to-one discussions. The need for concomitant medical therapy should be emphasized and the patient should understand that proper results take time (a few months to a year). Preoperative laboratory studies include hemogram including platelet counts, bleeding and clotting time (or prothrombin and activated partial thromboplastin time), and blood chemistry profile. Screening for antibodies for hepatitis B surface antigen and HIV is recommended depending on individual requirements. Anesthesia: Lignocaine (2%) with or without adrenaline is generally used for anesthesia; infiltration and nerve block anesthesia are adequate in most cases. General anesthesia may be needed in patients with extensive lesions. Postoperative care: Proper postoperative immobilization and care are very important to obtain satisfactory results. Keywords: Vitiligo, Skin grafting, Punch grafting, Suction blister grafting Introduction Vitiligo is a common acquired depigmentation disorder of great cosmetic importance. The basic pathogenesis of vitiligo or for any of the putative subsets of vitiligo, still remains unknown. The medical treatment of vitiligo is dependent upon the presence of a melanocyte reservoir and is effective in only 60-70% of the patients. Certain types of vitiligo do not respond well to medical treatment and resistant lesions do persist even in those who respond. In light of these limitations of medical treatment, surgical treatment of vitiligo was first proposed in the 1960s. Over the years, the concept of surgical treatment has been expanded to include surgical "biotherapies" such as autologous, cultured melanocyte transplantation. The disease has a major impact on the quality of life of patients, particularly the Indian population, in which there is a severe stigma attached to the disease, affecting the social and psychological aspects of the patients. Due to these effects, there is a considerable need for active treatment of this disease, in contrast to fair-skinned patients in whom the disease is less apparent.Rationale and Scope As such, there are no uniformly acceptable measurement tools and indices for measurement of the efficacy of outcomes of the surgical modalities of vitiligo treatment. Assessment of quality of life and global assessment should be performed because the percentage of regimentation may not always be a good indicator of patient satisfaction. There is an urgent need for universally acceptable, objective, reproducible and easy-to-use measurements to evaluate the efficacy of surgical vitiligo studies. These guidelines provide minimal standards of care for various surgical methods of treatment of vitiligo, with a brief description of the procedures as well as their advantages and disadvantages.Physician′s Qualifications The physician performing vitiligo surgery should have completed postgraduate training in dermatology; he/she should also have had adequate training in vitiligo surgery during postgraduation. Alternatively, training in vitiligo surgery may be obtained on the surgical table (hands-on) under the supervision of an appropriately trained and experienced dermatological surgeon. The training may also be obtained in dedicated workshops. In addition to the surgical technique, training should include techniques in local anesthesia and emergency resuscitation and care.Facility Vitiligo surgery can be performed safely in an outpatient day care dermatosurgical facility under local anesthesia. The day care theater should be equipped with facilities for monitoring and handling emergencies. A plan for handling emergencies should be in place with which all nursing staff should be familiar. Transplantation for extensive areas of vitiligo may need general anesthesia and in such cases, an operation theater facility in a hospital setting and the presence of an anesthetist are recommended.Indications for Surgery and Patient Selection Surgery is indicated for all types of stable vitiligo including segmental, generalized and acrofacial types that do not respond to medical treatment. While there is no consensus on definitive parameters for stability, various recommendations suggest a period of disease inactivity ranging from six months to two years. The task force agrees on a year of disease inactivity as the cut-off period for defining stability (Level D). Test grafting may be performed in doubtful cases to detect stability. The choice of surgical intervention should be individualized according to the type of vitiligo, stability, localization of lesions and cost-effectiveness of the procedure. Patient counseling about the nature of the disease and about the fact that the determination of stability is only a rough guide is essential.Explanation for Stability The outcome of surgery is good in stable lesions whereas unstable lesions respond poorly. Thus, the stability status of vitiligo is the single, most important prerequisite in case selection. However, despite many studies, there is no consensus regarding the minimum required period of stability. The recommended period of stability in different studies has varied from four months to three years. Most authors have suggested that vitiligo can be classified as being stable when there is no progression of old lesions and/or development of new lesions during the past one year. A set of objective criteria-the Vitiligo disease activity score (VIDA), was suggested by Njoo et al. (7) in 1999 to follow the progress of the patient. It is a 6-point scale on which the activity of the disease is evaluated by the appearance of new vitiligo lesions or the enlargement of preexisting lesions gauged during a period ranging from < 6 weeks to one year [Table - 1]. The task force recommends that surgery for vitiligo should be performed only in patients with VIDA scores of -1 or 0 (Level D). Evidence
In contrast, other authors have questioned the concept of stability and stated that existing parameters are arbitrary. Evidence
Parameters for Establishing Stability of Vitiligo
Consensus Recommendation of the Taskforce on Stability The available evidence is insufficient to recommend a single cut-off period to assess stability. To facilitate consensus on this issue, the task force attempts to provide a clear definition of stability-a patient reporting no new lesions, no progression of existing lesions, and absence of Koebner phenomenon during the past one year. Spontaneous repigmentation should be considered as a favorable sign for the transplantation procedure. A test graft may be considered whenever there is a doubt about the stability, or the patient is unable to give a clear history on stability. It needs to be stressed here that the treating physician should always consider each patient individually and exercise his/her judgment (LEVEL D). 2. The age of the patient for vitiligo surgery : As such, no uniformly accepted opinion exists concerning the minimum age for surgery. Vitiligo surgery is generally performed under local anesthesia, which would be difficult in children. General anesthesia for vitiligo surgery in a young child poses unacceptable risks and the progress of the disease is difficult to predict in children. Hence, many dermatologists feel that surgical procedures should not be performed in children. However, studies have suggested that results of transplantation procedures were better in younger individuals than in older ones. Thus, no consensus exists in this aspect and physicians should exercise their judgment after taking all aspects of the individual patient into consideration. (LEVEL C) Evidence
Preoperative Counseling and Informed Consent Proper counseling is essential; the nature of the disease, procedure, expected outcome and possible complications should be clearly explained to the patient. The need for concomitant medical therapy should be emphasized. Patients should understand that proper results may take time to appear (few months to one year). The patient should be provided with adequate opportunity to seek information through brochures, computer presentations, and one-to-one discussions. A detailed consent form (see appendix 1) describing the procedure and possible complications should be signed by the patient. The consent form should specifically state the limitations of the procedure, possible future disease progression and whether more procedures will be needed for optimal outcome. Anesthesia The recipient site is locally anesthetized by infiltration of 2% xylocaine, the pain of which can be reduced by prior application of EMLA ® cream applied under occlusion for 1-2 hours. Adrenaline should not be used on the recipient site as it makes the judgment of adequacy of the denudation to the required depth difficult. Tumescent anesthesia and nerve blocks may be used in larger areas. If grafting is planned for extensive areas, general anesthesia may be needed in a hospital setting. (LEVEL D)Methods of Surgical Modalities Methods of surgical modalities for vitiligo include both tissue grafts and cellular grafts.Tissue Grafts
Dressings are postoperatively placed to ensure immobili- zation, and may be removed in 24 hours to check for the displacement of the grafts. Grafts are taken up in 7-10 days after which phototherapy or treatment with topical steroid is started to ensure even spread of perigraft pigment. Evidence
Advantages : This is the easiest and least expensive method and may be used satisfactorily in all areas other than the nipples and the angle of the mouth, where involuntary muscle contraction may interfere with graft uptake. It is even suitable for ′difficult-to-treat′ locations such as the fingers, toes, palms and soles, etc. Disadvantages and complications : This method is not suitable for large lesions as uniform pigmentation may not always be achieved. Other important complications include cobblestoning and a polka dot appearance. 2. Suction blister epidermal grafting: This procedure consists of obtaining very thin skin grafts consisting of only the epidermis. A physiological split is made at the dermoepidermal junction by the application of prolonged suction at a negative pressure of -200 to -500 mm of Hg to the donor site. The recipient site is dermabraded by using either a manual or a motorized dermabrader, depending on the size and site of the lesion. Thin grafts are applied to the dermabraded recipient site. Alternatively, the recipient site may be denuded by an Erbium:YAG or carbon dioxide (CO 2 ) Laser. Equipment needed includes specially altered disposable syringes, suction cups or glass funnels, suction apparatus and manual/motorized dermabraders. The graft may fall off in a period of a week to ten days. (LEVEL B) Advantages: It yields excellent cosmetic results as the graft is very thin. One of the major advantages of this procedure is that chances of scarring at the donor or recipient sites are minimal as the graft is purely epidermal. Disadvantages : The major disadvantage of this procedure is that it is time-consuming as donor site blistering requires a few hours. Large areas can not be treated by this method. Evidence
3. Split-thickness grafting: Split-thickness skin grafting involves the free transfer of the epidermis along with a portion of the dermis from one site to another. The procedure is carried out under local anesthesia (for localized lesions) or general anesthesia (for extensive lesions). It consists of obtaining very thin, split thickness skin grafts, consisting of the epidermis and a part of the upper papillary dermis, and grafting them on the denuded (dermabraded or Laser-abraded) recipient site. The grafts are further secured with pressure and immobilization. Motorized dermatomes such as Padgett′s or Zimmer′s dermatomes, may be used to obtain ultra-thin, split-thickness grafts, which may give cosmetically superior results compared to those with manual dermatomes (Level B) . Instruments include dermabraders, skin-grafting knives such as the Humby′s knife or any of its modifications, as well as other surgical instruments. Large areas can be grafted in a single sitting. Advantages: This method has the advantage of treating a relatively large area in a short period of time. Disadvantages : Taking split-thickness grafts of uniform thickness requires skill and experience. Other disadvantages include ′stuck-on′ or ′tire patch′ appearance, curling of the border with beaded appearance, color mismatch, milia, perigraft halo of depigmentation, and donor site scarring. Evidence
4. Other tissue grafting procedures : Several other methods of tissue grafting have been performed by different authors. These methods or their modifications may be used by the treating physician depending on individual expertise and experience. Hair follicle-grafting has been performed by a few authors for treating small patches in hair bearing areas and has been found useful in treating lesions with leukotrichia. A small strip of hair-bearing scalp is taken from the occipital area; single hairs are separated and transplanted into vitiligo patches 5-10 mm apart. (LEVEL C) Evidence
In flip-top grafting, superficial, thinly shaved biopsies that are 2-4 mm in size, are taken using a razor blade, which are then sectioned into smaller 1-2 mm grafts. A 5-mm flap of epidermis with minimal dermis is raised with a razor blade at the recipient site, and the grafts are placed under this flap. The major advantage of this procedure is that there is rapid healing and no cobblestoning. (LEVEL C) Evidence
Cellular Grafts These methods represent important recent advances and need specialized training and appropriate equipments. The following cellular grafting techniques have been advocated in the surgical management of vitiligo:
1) Transplantation of autologous, epidermal cell suspension (noncultured melanocyte grafting): In this procedure, a shave biopsy sample is taken with a dermatome. The skin sample is immersed in a trypsin solution, the epidermis separated from the dermis, and after some additional steps, a cellular suspension of keratinocytes and melanocytes is obtained, which is transplanted on the denuded recipient site. (LEVEL B) Advantages : In comparison with other surgical methods, the basal layer suspension method has the advantage that a fairly large area can be treated with the donor-to-recipient expansion ratio ranging from 5-10 fold. (LEVEL B) Disadvantages: Taking split-thickness grafts requires skill and experience. This technique requires a properly equipped laboratory and trained personnel. Evidence
2) Transplantation of cultured autologous melanocytes: Melanocytes are cultured in vitro for 15-30 days by the addition of media and growth factors. Once sufficient numbers are present, melanocytes are detached from the culture plates and suspension is transplanted onto the denuded recipient area in a density of 1000-2000 melanocytes/mm 2 . The recipient area can be denuded by dermabrasion, CO 2 , or an Erbium:YAG Laser. (LEVEL B) Advantages : The major advantage is that the procedure can treat unlimited areas; however, it is recommended that vitiligo involving > 30% of the body surface area should not be treated surgically as chances of success are minimal in such cases. (LEVEL D) Disadvantages : There have been some safety concerns about the use of cultured autografts in vitiligo. 12-tetradecanoylphorbol 13-acetate (TPA) used in the culture medium is a tumor promoter, making its long-term safety a concern. But recent availability of TPA-free and serum-free media provide a solution to this problem. However, this method is expensive and requires a tissue culture laboratory setup. Evidence
3 ) Autologous cultured epithelial grafts: Cells are seeded in a medium that allows co-cultivation of keratinocytes and melanocytes. A few weeks later, a cultured epidermal sheet is obtained, released by dispase and attached to petrolatum gauze. The recipient site is prepared as described in the cultured melanocyte transplantation section and the gauze is applied on the recipient site and dressed. (LEVEL B) Advantages: The major advantage is that cells are expanded in the cell culture to treat a large area. Disadvantages: The technique requires special personnel and equipments and is expensive. Evidence
Certain Special Methods of Treatment in Selected Situations Tattooing has been recommended as a suitable method in the angle of the mouth. Dermabrasion and chemabrasion (with cauterants such as trichloroacetic acid/phenol) have been used in lesions on hairy areas to produce pigmentation as adjuvant to phototherapy. A 308-nm excimer Laser has been found to be successful in a few studies, with > 75% repigmentation occurring in about 30% of the patients; it is not effective in acral areas. (LEVEL C) Evidence
Evidence-Based Practice Guidelines for Choice of Method As already highlighted, there is no uniformly acceptable objective measurement tool to compare the surgical outcome of a given modality. Recently, an attempt has been made by the European Taskforce on vitiligo to define and assess the severity of vitiligo. A scoring system has also been suggested to evaluate the outcome of transplantation procedures in vitiligo, although it is mostly subjective and has not been validated for interobserver bias in a large sample size. (LEVEL C) Evidence
Various meta-analyses of published studies have shown that split-thickness grafting, suction blister epidermal grafting, and punch grafting have comparable success rates of repigmentation. (LEVEL A) Evidence
Similarly, all three cellular graft techniques (non-cultured epidermal cell suspension, cultured melanocytes and cultured epidermis) were found to be equally effective. However, in comparison to tissue grafts, cellular grafts showed slightly lower success rates. One explanation may be that cellular grafts are generally used to treat larger areas in comparison to tissue grafts. (LEVEL A) Evidence
When compared on the basis of adverse events, the highest incidence of adverse events was reported with punch grafting followed by split-thickness grafting and suction blister epidermal grafting. Cellular grafting was associated with the lowest number of adverse events. Evidence
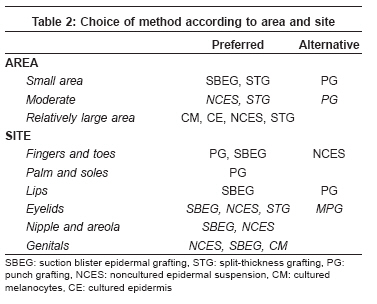
Conclusion Surgical methods of treatment for vitiligo constitute an important adjuvant for medical therapy. Proper case selection based on the determination of stability of the lesions is very important but no uniform criteria exist for the determination of stability. Hence, in an attempt to build consensus on this issue, the task force suggests the following definition of stability: a patient reporting no new lesions, no progression of existing lesions, and absence of Koebner phenomenon over the past one year. Above all, proper patient counseling about the nature of the disease and the surgery is essential. Recommendations for the choice of surgical method for different types, sites, and areas are shown in [Table - 2] (Level D).Acknowledgment The authors are indebted to Dr Koushik lahiri′s and Dr Lt Col Manas Chatterjee for their inputs while preparing these guidelines.Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08140t1.jpg] [dv08140t2.jpg] |
| |||||||||

{kind=link}
{kind=link}