 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
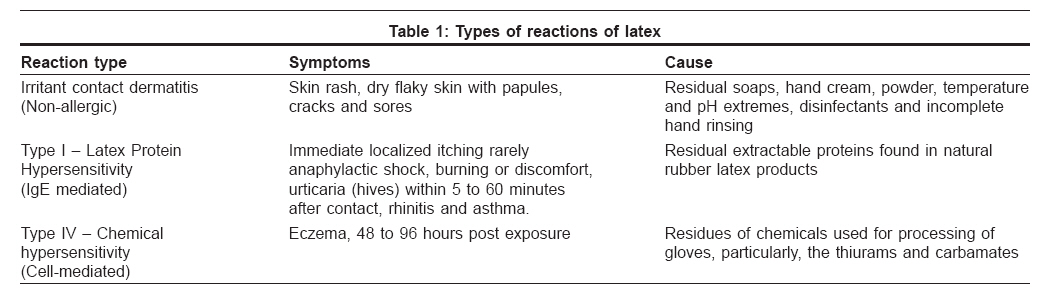
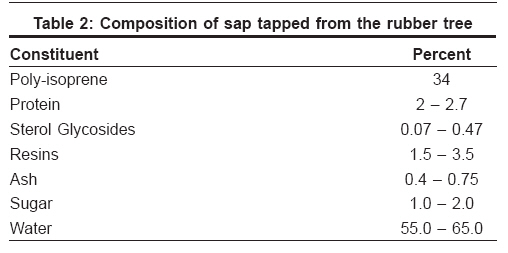
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 304-310 Review Article Natural rubber latex allergy Deval Ravi, Ramesh V, Prasad GBKS, Jain ArunKumar Institute of Pathology (ICMR), New Delhi Code Number: dv08147 Abstract Natural rubber latex (NRL) is a ubiquitous allergen as it is a component of > 40,000 products in everyday life. Latex allergy might be attributed to skin contact or inhalation of latex particles. Latex allergy is an IgE-mediated hypersensitivity to NRL, presenting a wide range of clinical symptoms such as angioedema, swelling, cough, asthma, and anaphylactic reactions. Until 1979, latex allergy appeared only as type IV delayed hypersensitivity; subsequently, the proportion of different allergy types drifted towards type IV contact allergy reactions. Several risk factors for sensitization to NRL are already known and well documented. Some authors have established a positive correlation between a history of multiple surgical interventions, atopy, spina bifida malformation, and latex allergy incidence. We suspect an increase in latex allergy incidence in association with increased atopy and sensitivity to environmental allergens in the industrial population. It is often postulated in literature that the groups of workers at risk for this allergy are essentially workers in the latex industry and healthcare professionals. In this population, direct internal and mucosal contact with NRL medical devices may be the route of sensitization as factors such as the number of procedures and use of NRL materials (catheters and tubes) were associated with increased risk of latex sensitization and allergy. Keywords: Allergen, Hypersensitivity, Natural rubber latex Introduction During the 1980s and the 90s, allergy to natural rubber latex had posed serious concerns, particularly in certain occupational groups exposed to latex allergens. [1],[2],[3],[4] Natural latex is a milky sap produced by many different plants. However, the latex that is used industrially is derived almost exclusively from the rubber tree, Hevea brasiliensis, which belongs to the family Euphorbaceae. This liquid sap is processed to make many rubber products used in the home as well as at workplaces, such as: balloons, rubber toys, pacifiers, baby-bottle nipples, rubber bands, adhesive tape, bandages, diapers, sanitary pads, condoms, etc. In addition, many medical and dental supplies contain latex including gloves, urinary catheters, dental dams and material used to fill root canals, as well as tourniquets and equipment for resuscitation. Latex is composed of spherical poly-isoprene droplets coated with a layer of water-soluble proteins. [5] Natural rubber ( cis -1,4-polyisoprene) is a processed plant product of the commercial rubber tree, Hevea brasiliensis . It contains variable amounts of water-soluble proteins that can be recognized as allergens by the human immune system. [6] Allergy to latex was first recognized in the late 1970s. Since then, it has become a major health concern as an increasing number of people in the workplace are affected by latex. Healthcare workers exposed to latex gloves or medical products containing latex are especially at risk. What is Latex Protein Allergy? Latex concentrate contains about 1% total protein, a small fraction of which remains in the resulting manufactured product as residual extractable protein. This protein material binds to a specific human IgE antibody and has been implicated in severe allergic reactions. By contrast, dry rubber contains very little protein and is therefore much less immunogenic than latex sap. [7] Latex gloves cause both allergic and nonallergic symptoms to different rubber products as detailed in [Table - 1]. While irritant contact dermatitis and Type IV hypersensitivity have been known for many years Type I hypersensitivity emerged only in the late eighties. It may be worth noting that Type I hypersensitivity is not confined to natural rubber latex (NRL) products. Individuals may initially present with signs and symptoms of contact dermatitis and later with continued exposure, demonstrate potentially more severe signs and symptoms of immediate hypersensitivity mediated by IgE. Who is at Risk for Latex Protein Allergy? Latex allergy is reported more frequently among those heavily exposed to NRL products such as: healthcare workers, janitorial staff, hairdressers, and rubber industry workers. [8] Latex sensitization can occur not only through direct contact of an NRL-containing product with the skin ( e.g ., gloves) but also via mucosal ( e.g ., catheters, condoms) or parenteral routes. One of the most efficient sources of sensitization in a medical or dental environment is via aerosolized latex protein from powdered latex gloves. Powder, which is commonly used as a dry lubricant on disposable latex gloves, is an excellent carrier of allergenic latex proteins. Individuals who have undergone multiple surgical or dental procedures are also at high risk. Children with neural tube defects (spina bifida, meningomyelocele) also have a high prevalence of latex allergy. [9],[10] Direct internal or mucosal contact with NRL devices appears to be an important route of sensitization in these patients as well as for those with congenital urologic abnormalities. Lastly, persons with atopy are also at increased risk, along with those with preexisting hand dermatitis. Signs and Symptoms of Latex Allergy An immediate allergic reaction may occur within minutes of coming into contact with latex. Symptoms of a reaction include hives, wheezing, coughing, shortness of breath, sneezing, nasal congestion, runny nose, conjunctivitis, nasal, palatal, or ocular itching, urticaria, naso-rhinitis, asthma and hypotension. [11],[12],[13],[14],[15] Hives can appear anywhere on the body and not necessarily at the point where direct contact with the latex occurred. Immediate reactions can be life-threatening when blood pressure drops, airways blocked, and the throat closes. [16] This condition can eventually progress to anaphylaxis. [17],[18],[19],[20] These symptoms can be exacerbated in certain people when specific foods are ingested due to cross-allergenicity. [21],[22] A person who comes in contact with latex may sustain a mild allergic reaction. However, when ingesting a cross-reacting food later, new reactions can occur within 5-30 minutes, resulting in itching and irritation of oral tissues, swelling of the lips and tongue, and sometimes papules or blistering of these tissues. [23]Other Associated Allergies Allergy to latex rubber involves sensitization to multiple constituent proteins. Therefore, different groups of patients respond to specific latex proteins in various ways. [24],[25] These groups of proteins are found in many products including, but not limited to, certain tree pollens, some plants, and (most commonly) fresh fruits. [23],[26] Fresh fruits that commonly cause hypersensitivity when associated with latex proteins are avocado, banana, celery, chestnut, and pear. Less common are apricot, buckwheat, cherry, fig, grape, kiwi, mango, melon, nectarine, orange, papaya, passion fruit, peach, peanut, pineapple, plum, potato, tomato, and walnut. [22],[27],[28] The problem manifests itself in two ways: (1) the fruit allergy triggers previously undiagnosed recognition of the latex allergy or (2) after years of latex exposure and latex sensitivity, the person develops fruit allergies. Whether this dual latex-fruit sensitivity is determined by common antigens or cross-reacting antigens has yet to be determined. [24],[25]Global Prevalence of Latex Allergy In recent years, allergy to NRL has emerged as a major allergy among certain occupational groups and patients with underlying diseases such as acquired immune deficiency syndrome (AIDS) and other viral infections. The sensitization and development of latex allergy has been attributed to exposure to products containing residual latex proteins. [29] Most epidemiological studies show a sensitization prevalence of around 5-17 and 3.7-8.0% in healthcare and rubber industry workers, respectively. [30],[31],[32],[33] Sensitization prevalence is 12.5, 18-37 and 34-67% among anesthesiologists, [35] individuals who have undergone multiple surgical procedures [36],[37],[38] and children with neural defects, respectively. [9],[10],[39] Lastly, persons with atopy (atopic eczema, allergic rhinitis, hay fever, or asthma) are also at notably increased risk along with those with preexisting hand dermatitis. [40] Reports of immediate hypersensitivity to latex have increased dramatically since the first case was reported by Nutter. [41] In 2005, Johar et al , [42] investigated the prevalence of latex allergy in a cohort of 24 children suffering from spina bifida in South Africa and found latex sensitization in 16.7% of the cases. Khader et al , [43] reported the prevalence of latex (gloves) allergy among healthcare workers in Jordan to be 13.6%. [43] In the same year, Proietti et al, [40] studied latex allergy among healthcare workers and observed that 60 subjects were associated with work-related symptoms, and 35 (2.7%) out of these 60 subjects, who were also atopic, had latex allergy. This study confirmed that atopy is an important factor that should be considered as a risk for the development of latex allergy. In an another study in Trieste, Filon and Radman [44] concluded that unnecessary glove use, the use of non-powdered latex gloves by all healthcare workers, and the use of non-latex gloves by sensitized subjects could restrict the progression of latex symptoms, and could avoid new cases of sensitization. Natural rubber ( cis -1,4-polyisoprene) is a processed plant product of the commercial rubber tree, Hevea brasiliensis . It contains variable amounts of water-soluble proteins that can be recognized as allergens by the human immune system. [6] Despite this recognition, latex allergy remains the second most common cause of intra-operative anaphylaxis, [45] and one in fifty healthcare workers becomes sensitized to latex each year through exposure to latex gloves. [35],[46] Adverse reactions due to latex products have recently been documented by Huber and Terezhalmy, [47] and researchers have emphasized its key role in allergenicity. [48] Koh et al , [49] investigated the amounts of specific allergens found in rubber gloves that cause NRL allergy. They found that NRL allergen levels were high in the majority of examination gloves used by healthcare workers and thus, were more likely to cause NRL allergy among sensitized persons. Crippa et al , [50] investigated latex protein content in different medical devices and devices commonly used in general practice to acquire information for the prevention of latex allergy among healthcare workers and in the general population. A high level of latex protein was found in medical devices such as elastic bandages (81.57%), tourniquets (74.09%), Foley′s urinary catheters (68.35%), Penrose drainage (67.25%) and taping (39.6%), and in common devices, such as rubber inner-soles (84.20%), toy balloons (78.62%), latex mattresses (74.27%), household rubber gloves (49.10%), working gloves (38.25%), and inflatable floating mattresses (32.10%). They concluded that every natural rubber object should be systematically labeled as "containing latex" along with the warning that "this item may cause allergic reactions in sensitized subjects". In 1998, the United States Food and Drug Administration (FDA) mandated that products that contain latex be labeled as such. [51] Products can no longer be labeled as "hypoallergenic" because the FDA has received several reports of allergic reactions to medical gloves labeled in this way. The FDA also requires labeling of dry natural rubber although this type of rubber is less allergenic. The FDA ruling also mandates that nonmedical devices that make contact with human skin/tissue such as adhesives used on Band-Aids, also be labeled. In the last few years, latex allergy has been recognized as a potential medical problem in India. Latex allergy is reported more frequently among those heavily exposed to NRL products such as latex gloves and other medical supplies used by healthcare workers as well as household gloves, elastic bandages, condoms, envelop adhesive, rubber bands, infants′ and children′s bottle nipples etc used by housekeepers, latex industry workers, and food service workers. However, latex allergy has received very little attention in Indian studies as evidenced by the absence of scientific, practical, and systematic data on the subject. Pherwam et al , [52] reported latex sensitivity among operation theater personnel in India and found nurses and ward boys to be the most susceptible to sensitization in comparison to surgeons and anesthetists, but the sample size was too small to draw any further conclusions. Manufacture of Latex Manufacturers have produced latex gloves for over 100 years and are now aware of the increase in allergic problems due to latex. It is estimated that 2, 50, 000-5,00,000 healthcare workers are now sensitized to latex protein in the US alone. There are more than 30 companies that manufacture gloves and their leaching and washing requirements may be reduced or eliminated. Thus, residual accelerators and water-soluble proteins are not removed from the gloves, which in turn results in sensitization to latex. The composition of the milky white sap that is tapped from the tree is detailed in [Table - 2]. Accurate measurement of the protein in latex medical products is difficult, especially as the chemical additives to the latex interfere in protein estimation assays. [53] Most of the proteins are water-soluble and readily leach out of the latex, but complete extraction is possible overnight. It is now established the proteins in natural rubber latex and their derivatives are the causes of NRL allergy. The corn starch procedure used for manufacturing of the latex gloves does not itself contain allergenic components, but acts as a carrier for latex proteins. Eleven latex proteins have been registered as latex allergens by WHO. Diagnosis of Latex Allergy Preparation of latex allergens from gloves Skin prick test (SPT) Nutter [41] was probably the first to describe a positive skin test to latex and used 5% of natural latex which had been extracted over a period of 24 hours. Later on, Turjanmaa et al , [56] were the first to show that extracts of latex gloves can cause positive skin prick test (SPT) reactions in patients who are allergic to NRL. Intradermal test (ID test) The test should be performed in a facility with emergency medical equipment available to handle an anaphylactic reaction. [57],[58],[59] In vitro laboratory tests There are many substances in rubber that can cause delayed type IV response and patch testing may be necessary to confirm the skin reaction. Also, immediate and delayed reactions may occur in the same subject. [60] Contact test Avoidance and Education Programming and education To help reduce the occurrence of latex allergies among healthcare workers and patients, the American College of Allergy, Asthma, and Immunology has established new practice guidelines: [64]
Treatment Patients who are known to be allergic should avoid any product that might contain latex until the latex content is determined by contacting the manufacturer. Even products labeled "safe latex" (which indicates lower proportions of natural latex) can cause latex allergy. There is no safe latex for latex allergy sufferers. Although medications are available to reduce the symptoms of latex allergy, no cure for latex allergy exists. Type I reactions are treated as any other systemic allergic reaction. The cornerstones of treatment are epinephrine and antihistamines (H1 antagonists); systemic corticosteroids and H2 blockers may be useful. Type IV reactions (localized contact dermatitis) can be treated with topical steroids along with patient education to avoid further exposures. Alternatives to Latex Avoidance of the provoking agent (latex allergen) is the most effective way to manage any allergy. Latex-free synthetic rubber such as neoprene, nitrile, styrene butadiene rubber (SBR), butyl and vitron are polymers that are available as alternatives to natural rubber. There are no naturally occurring proteins in them and they are not responsible for latex allergy. Labeling is extremely important, but mandatory labeling is currently not required by law.Resource Information Several websites offer information on latex allergies, including current clinical management and prevention of allergic disorders. Answers to frequently asked questions, educational resources, and alternative products are available. [67]
References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08147t2.jpg] [dv08147t1.jpg] |
| |||||||||

{kind=link}
{kind=link}