 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
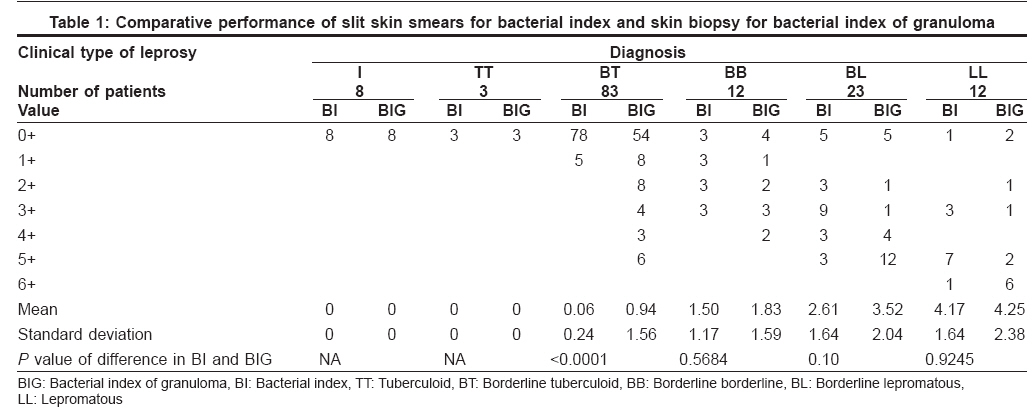
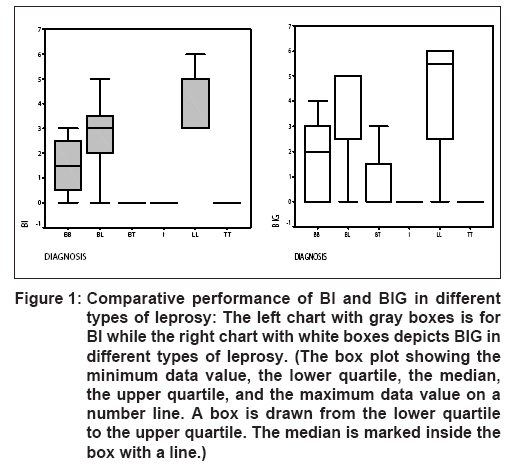
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 322-326 Original Article Diagnosing multibacillary leprosy: A comparative evaluation of diagnostic accuracy of slit-skin smear, bacterial index of granuloma and WHO operational classification Bhushan Premanshu, Sardana Kabir, Koranne RV, Choudhary Monisha, Manjul Prateek Departments of Dermatology, Leprosy and Sexually Transmitted Diseases, Lady Hardinge Medical College and Associated Hospitals, New Delhi Code Number: dv08149 Abstract Background: In view of the relatively poor performance of skin smears WHO adopted a purely clinical operational classification, however the poor specificity of operational classification leads to overdiagnosis and unwarranted overtreatment while the poor sensitivity leads to underdiagnosis of multibacillary (MB) cases with inadequate treatment. Bacilli are more frequently and abundantly demonstrated in tissue sections.Aims and Methods: We compared WHO classification, slit-skin smears (SSS) and demonstration of bacilli in biopsies (bacterial index of granuloma or BIG) with regards to their efficacy in correctly identifying multibacillary cases. The tests were done on 141 patients and were evaluated for their ability to diagnose true MB leprosy using detailed statistical analysis. Results: A total of 76 patients were truly MB with either positive smears, BIG positivity or with a typical histology of BB, BL or LL. Amongst these 76 true-MB patients, WHO operational classification correctly identified multibacillary status in 56 (73.68%), and SSS in 43 (56.58%), while BIG correctly identified 65 (85.53%) true-MB cases. Conclusion: BIG was most sensitive and effective of the three methods especially in paucilesional patients. We suggest adding estimation of bacterial index of granuloma in the diagnostic workup of paucilesional patients. Keywords: Bacterial index, Bacterial index of granuloma, Leprosy diagnosis Introduction The sixth WHO expert committee report in 1988 recommended all smear positive leprosy cases be treated as MB patient [1] which was later changed to a purely clinical classification with patients having> 5 skin lesions considered MB and ≤5 as PB. [2] However, such purely clinical classification leads to a small but significant number of MB cases being treated with PB regimen. [3] The specificity of slit-smears is almost 100% as it directly demonstrates the presence of acid-fast bacilli (AFB) but the sensitivity is low and varies from 10-50%. [3] Histological examination has many advantages and the yield of AFB in tissue sections are reported to be better. [4],[5],[6] The study was designed to compare the efficacy of bacterial index (BI) in SSS and BIG in biopsies for detecting the truly MB cases and the relative performance of WHO operational classification, SSS and BIG in tissue sections in this respect.Methods We studied 150 consecutive and untreated cases of leprosy at the Department of Dermatology, Lady Hardinge Medical College and associated hospitals, New Delhi. Patients who had received any specific therapy for leprosy in the past, those who had pure neuritic leprosy or those who did not give consent were excluded from the study. Patients were clinically classified based on number, type and characteristics (including grade of sensory loss, borders, dryness, scales, hair-loss etc.) of skin lesions and nerve involvement; into indeterminate (I), tuberculoid (TT), borderline tuberculoid (BT), borderline borderline (BB), borderline lepromatous (BL) and lepromatous (LL) leprosy. Patients were also classified as PB or MB based on the number of skin lesions. Three slit skin smears, two from the representative lesions and one from an earlobe were obtained and stained by Ziehl Neelsen method. At least 100 oil-immersion fields of the smears were examined by at least two investigators for the presence of AFB and BI was calculated. Skin biopsies from most representative lesions were stained by both hematoxylin and eosin as well as modified Fite method [7] for AFB. [7] A minimum of three complete tissue sections were examined by at least two of the investigators for histopathological changes and for calculation of the BIG in them. [8],[9] For both BI and BIG calculation two investigators examined the slides simultaneously and a consensus value was taken. We did not analyze for inter-observer variations. Patients who demonstrated AFB in SSS or biopsy as well as those with a typical histology of BB, BL or LL were considered true- MB patients. [5] The data thus obtained was pooled and analyzed with Statistical Package for Social Sciences (SPSS TM for Windows TM V 9.0.0, SPSS, Inc.) and Smith′s Statistical Package TM V 2.75. Results Study group Clinical features Skin slit smears Histological examination BIG in tissue sections Comparison of SSS and BIG [Table - 1] and [Figure - 1] The difference between the values of BIG and BI varied from 0 to 6. The mean difference between the values of BI and BIG was higher than BI in all and it was least in LL [0.08 (± 0.71)] and maximum in BL [0.91 (± 0.55)]. The difference between the values (bacterial yield) of BI [mean: 0.943; SD: 1.638] and BIG [mean: 1.645; SD: 2.098] was statistically analyzed with paired-t-test and was found to be highly significant (p < 0.0001). Furthermore, the difference was highly significant in BT patients with p < 0.0001). It was also observed that 33 (76.74%) out of 43 SSS positive cases were also positive for BIG. In contrast, SSS was positive only in 33 (50.77%) out of 65 patients who were BIG positive and the difference was again significant (Chi-square test, p< 0.001). The SSS were positive in 2(2.98%) of the 67 WHO-PB patients [1 SSL and one with 2-5 lesions] as compared to 18 (26.87%) BIG positive patients [5 SSL and 13 with 2-5 lesions] and the difference was significant ( z-test; p< 0.05). Again, BIG was positive in 47 of 74 (63.51%) WHO-MB patients as compared to 41 (55.40%) SSS positive cases however, the difference was statistically not significant. Amongst 26 highly bacillated patients, i.e., with a BIG of 5-6+, SSS were positive for AFB in 17 (65.38%) patients. On the other hand, for BIG values of 1-4+ the SSS were positive in 16 out of 39 (41.02%) patients. Since SSS was going to be more positive in highly bacillated patients only, one tailed Fisher′s exact test [10] was conducted and the difference was statistically significant (p< 0.05). Therefore, at low tissue bacillary density BI was far less effective in demonstrating AFB. Performance of WHO classification as compared to SSS and BIG WHO classification alone, correctly classified 56 of 76 true- MB patients with a sensitivity of 73.68% and specificity of 72.31%. Thus 26.32% patients were misclassified as PB. The PPV of WHO system was 75.68% and the NPV was 70.15%. The McNemar′s tests [10] for the differences between sensitivities of SSS, BIG and WHO system were significant ( p0 < 0.001). Interestingly the WHO classification classified 18 (27.69%) of 65 true- PB patients as MB thus leading to overdiagnosis. WHO classification in conjunction with SSS would still have misclassified 18 of 76 true MB patients as PB i.e., skin biopsies and BIG identified 23.68% of misclassified PB cases as true -MB cases. Further, the concordance between BIG, SSS and WHO system to correctly identify true -MB patients was evaluated by the Cohen′s Kappa coefficient [10] and concordance was deemed to be mediocre when it was < 0.40 and good when ≥0.60. The Cohen′s Kappa coefficient was 0.845 for BIG, 0.546 for SSS and 0.459 for WHO classification. The mean BI in true- MB patients was 1.75(± 1.89) while the mean BIG in true- MB patients was 3.05(± 1.97). The difference between the mean BI and BIG was analyzed with two sided t test and the result was statistically significant (P< 0.001). Discussion Demonstrating AFB is still considered important for diagnosis, classification and management of leprosy. [11],[12] However, the sensitivity of SSS is poor (10-50%) [3] and it has been described as the weakest link. [13] To overcome the shortcomings of smears, WHO proposed a purely clinical classification. [2] Despite routine use, this classification has reported sensitivity from 85-93% with specificity of 42-88%. [14],[15],[16],[17],[18],[19] Further addition of more clinical criteria does not increase the sensitivity and specificity. [18],[19] While AFB are better demonstrated in biopsies, [4],[5],[6] it is technically demanding, invasive and has no definite role in management of leprosy. The reducing prevalence of leprosy entails an incremental involvement of higher centers. [2],[6] We evaluated whether additional information from BIG would increase the diagnostic accuracy in identifying MB patients. In our study significantly more patients were identified as MB with BIG(46.09%) as compared to SSS(30.50%). This BIG positivity in SSS negative patients is explained by the presence of AFB in deep reticular dermis where they remain inaccessible to SSS. [20] Similar findings of better performance of biopsy were reported in various studies. [6],[21],[22],[23],[24] We have demonstrated that this high positive BIG is also significantly seen in paucilesional, clinically BT and WHO-PB patients. Ponnighaus et al, reported finding 2 of 61 SSL patients with AFB-negative smears yet positive biopsies. [25] Similar observation was made by Srinivaas et al, [6] Our analysis reconfirmed earlier findings that in highly bacillated patients, SSS is quite sensitive but not in patients with low tissue-density of AFB. [6],[25] Therefore, SSS has significant underdiagnosis of true -MB patients. However, in 5 (11.63%) of our SSS positive patients BIG was negative. Groenen et al, also reported that 15% of patients were BI positive but BIG negative. [5] The explanation for this contradictory observation is that bacilli in biopsy may be missed because the biopsy is taken at the wrong spot or because the bacilli are concentrated in one specific area but the biopsy slices do not include the area. [26],[27] SSS in our study had a low sensitivity and NPV as compared to BIG. Such low sensitivity of SSS has been deliberated before, [3],[18] while poor NPV indicates a large proportion of patients being misclassified as PB. Such poor performance of SSS at a tertiary center underscores the importance of WHO classification, as poorer results would be expected in peripheral centers. Our analysis revealed the sensitivity to be higher with BIG as compared to WHO scheme or SSS. Further, the WHO system lead to overdiagnosis in 18 (27.69%) of 65 true-PB patients. Therefore, WHO system is significantly more sensitive than SSS but less than BIG and has the drawback of significant underdiagnosis as well as overdiagnosis. Many studies have demonstrated the sensitivity of WHO operational classifications ranging from 85-92% [14],[15],[16],[17],[18],[19] but many of these high values were observed using slit-smear as the "gold-standard". [14],[15],[16],[18] Ideally a skin or nerve biopsy should have been included to make diagnosis of true- MB leprosy. [5],[19] WHO system increases the sensitivity significantly as compared to SSS, but at a cost of a poor specificity as reported to be 41.3% by Groenen et al . [5] Even a combination of SSS with WHO operational classification added little to the sensitivity and still resulted in 23.68% underdiagnosis of true -MB cases as compared to BIG. The concordance analysis also demonstrated that BIG most closely approximated the true- MB status compared to SSS and WHO classification. Thus, WHO system is better than over-reliance on SSS, but still leads to significant underdiagnosis, undertreatment and consequent risks of resistance, relapses and progressive horizontal transmission. This is especially true of paucilesional patients and clinically BT patients. BIG is the most superior method for detecting AFB in leprosy patients and most closely resembles the true bacteriological status. We propose that in view of good sensitivity of WHO classification for patients with > 5 lesions, it may be worthwhile to consider doing histological analysis and BIG estimation in paucilesional patients, if the facilities are available. Importantly, one does not need to count the bacilli for managing patients and finding even one AFB in tissue section will be enough to consider a patient as MB, thus making the process easier. Conversely, the need for BI/BIG estimation can be done away with, if a uniform-MDT with three drugs were accepted in control programmes. [28] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08149t1.jpg] [dv08149f1.jpg] |
| |||||||||

{kind=link}
{kind=link}