 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
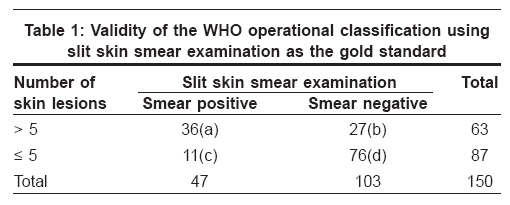
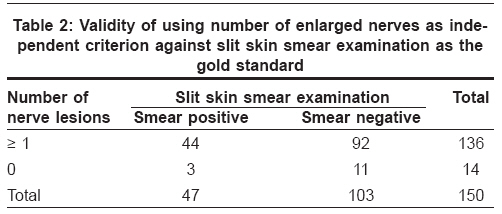
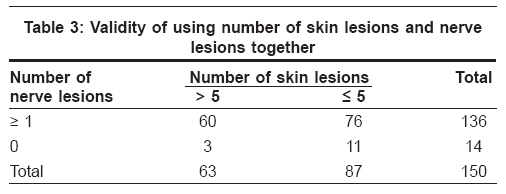
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 327-330 Original Article Does nerve examination improve diagnostic efficacy of the WHO classification of leprosy? Mehndiratta Ruchika Chandna, Patnaik Aurpit, John Oommen, Rao PSS The Leprosy Mission, Research Resource Centre, Noida, UP Code Number: dv08150 Abstract Background: In the year 1998 WHO proposed that the clinical criteria of counting skin lesions alone should decide whether a patient receives Multibacillary (MB) or Paucibacillary (PB) MDT. There is a concern that a significant number of patients may be incorrectly treated under these guidelines. Aims: This study aims to determine whether the sensitivity and the specificity of the latest WHO criteria, can be enhanced by the addition of nerve examination in the place of slit skin smears.Methods: 150 patients of untreated leprosy reporting at a TLM Hospital in Delhi from January to December 2006 were registered for the study. After physical examination, the number of skin lesions and nerves involved were counted and slit skin smears performed. Two groups were created, those with > 5 skin lesions, and those with 5 or less skin lesions. The diagnostic efficacy of the current WHO classification was calculated with and without the addition of nerve examination. Results: The sensitivity and the specificity of the current WHO operational classification are 76.6%, and 73.7% respectively, using slit skin smear as a standard. When the number of nerves was added to the diagnosis, the sensitivity increased to 94.4%, for more than 5 lesions and to 90.9%, for five or less than five lesions. Conclusions: Nerve examination can significantly improve the sensitivity of the WHO criterion in determination of MB versus PB leprosy. Keywords: Diagnosis of leprosy, Nerve enlargement, World Health Organization criteria Introduction Leprosy patients are classified into Paucibacillary (PB) and Multibacillary (MB) types based on the number of skin lesions, with five skin lesions being the "cut-off", and the treatment duration is determined based on this classification. [1] The World Health Organization (WHO) study group on the Chemotherapy of Leprosy in 1993 recommended that clinical criteria might be required for classification of the disease where facilities for bacteriological examination of skin smears were either unreliable or unavailable. [2] The WHO expert committee concluded that patients could be classified according to the number of skin lesions into three groups namely, paucibacillary single lesions (PB), paucibacillary (PB) (2 to 5 skin lesions), multi bacillary leprosy (MB) (6 or more skin lesions). [3] Several studies have reported the validity of these clinical criteria using skin smear as the gold standard. In the published studies, the sensitivity of the clinical classification ranged from 85% to 93% and the specificity from 39% to 88%. [4],[5],[6],[7],[8] There is a concern however, that by classifying patients exclusively on the number of skin lesions, a small but significant number of MB patients may wrongly receive PB treatment and fairly large number of PB patients would be treated unnecessarily with MB regime. [6] Using skin smear positivity as the gold standard, this paper reviews the sensitivity and specificity of classification based exclusively on counting the number of skin lesions. It also evaluates the possibility of replacing the slit skin smear by counting nerve lesions for the purpose of diagnosis and classification. Methods All new, untreated leprosy patients who presented at The Leprosy Mission (TLM) Hospital, Shahdara in the year 2006 were included. All defaulters and previously treated patients were excluded. These patients were screened at the out patient department by the principal investigator. A detailed clinical and physiotherapy assessment were carried out and all the patients were subjected to slit skin smear examination prior to the start of MDT. The clinical assessment included body charting of the patient was carried out by a trained MPW (multi purpose worker), which provided the details of the number and extent of skin lesions. A trained and qualified physiotherapist carried out the physiotherapy assessment. Enlargement in any degree of one of the nerves was regarded as a "nerve lesion" and noted. The details of nerve enlargement were obtained from the physiotherapy assessment sheet. A slit skin smear examination of all patients was carried out according to hospital protocol by a trained and qualified laboratory technician. The bacteriological index was obtained from the laboratory investigation sheet. The data collected was entered and analyzed using SPSS version 10.0. The sensitivity and the specificity of the WHO criteria were determined using the slit skin smear as a gold standard. The results were then reanalyzed with the addition of the findings of nerve examination. Results A total of 150 new untreated leprosy patients were registered in 2006. The information on the number of skin lesions and number of enlarged nerves was available for all of the patients. The mean age of these patients was 31.10 years with a standard deviation of 14.92 (Range - 7 to 85 years). Of these patients, 113 (76.9%) were male and 34 (23.1%) were female. The patients were grouped into two classes according to the WHO operational classification: those with > 5 skin lesions, and those with 5 or less skin lesions. Patients with diffuse infiltration of the skin, with thickened earlobes or with nodules were included in the former group (> 5 skin lesions). [9] [Table - 1] shows the correlation of the number of skin lesions (divided into the above mentioned 2 groups) and the slit skin smear examination (bacteriological index). A total of 5 patients had a single lesion of leprosy. From [Table - 1], the sensitivity of the current WHO operational classification that classifies a patient with greater than 5 skin lesions as MB, is 76.6%, while the specificity is 73.7%. The positive predictive value (PPV) is 57.1% and the negative predictive value is 87.3% [Table - 1]. There were 11 smear positive patients who presented with ≤ 5 skin lesions and would have been classified as PB according to the WHO classification, a false negative (false PB) rate of 23.4%. Among the 103 who were skin smear negative, 27 were found to have 6 or more skin lesions and hence would have probably been classified as MB, a false positive (false MB) rate of 26.2%. Thus only 112 (74.6%) patients were correctly classified as either MB or PB. We then evaluated the validity of nerve examination as an independent criterion against skin smear results for all patients and the findings are given in [Table - 2]. [Table - 2] shows that 44 patients were correctly classified as MB when the nerve lesions alone are used. The sensitivity is 93.6%, however the specificity is only 10.6%. The false positive rate (false MB) is 89.9% but a false negative (false PB) rate of 6.3%; the Positive predictive value is 32.3% but the negative predictive value is 78.5%. Thus the above results show that of the 47 patients who are smear positive, 44 have a nerve lesion and would be given MB.MDT. When nerve examination alone is used to classify patients, only 3 smear positive patients would have failed the gold standard. Under the current guidelines of WHO, smear examination is not recommended as a routine investigation. However, if only skin lesions are used to classify patients, 11 patients fail the gold standard and would be incorrectly treated. Hence we combined the two clinical parameters and evaluated the error rates when skin examination is combined with nerve examination to determine accurate treatment classification in [Table - 3]. Under the assumption that if a patient has a nerve lesion or if there are more than 5 lesions, the patients would receive MB.MDT, [Table - 3] shows 139 patients should receive MB.MDT and only 11 patients should receive PB.MDT. Out of 150 patients, 76 patients, who would have been classified as PB under the WHO guidelines, would now receive MB if nerve lesions are also taken into account. Thus skin examination alone may miss out on this group; of whom 10 would also have been smear positive. Nerve examination failed to detect 3 patients who fulfill the WHO criteria of MB. Out of these, only one patient was smear positive. 11 patients (7.3%) are now designated as true PB using both these parameters. Of these 11, only one patient was smear positive. The error rate of nerve examination in the detection of MB cases is 2.1% and that of skin lesions alone is much higher, i.e. 54.4%. But when the two are used together, the error rate falls to less than 1% (calculated value: 0.6%). Thus the chances of missing an MB patient are very low when both clinical parameters are used together. Discussion The criteria by which leprosy patients have been classified into PB or MB have changed considerably over the years. At the time of introduction of MDT in 1982, a revised and simplified classification into two groups, multibacillary (MB) and paucibacillary (PB) was put into practice. Using skin-smear results, a patient was classified as MB when the bacterial index (BI) was> 2+. [10] This was revised by the World Health Organization (WHO) Expert committee in 1988 by which the finding of a positive smear at any site led to MB classification. [11] In 1993 the WHO Study Group suggested that clinical methods alone could be used for classification where facilities for skin smears were unavailable or unreliable. [3] The latest recommendation by WHO divides the patients solely on the basis of counting the number of skin lesions. [3] This process does away with the making of slit skin smears that have been found to be the weakest link in the leprosy elimination program. [12] While this may be easier to apply in practice, there is a serious concern that a significant number of PB patients may receive MB treatment and vice versa. The benefits of being able to reach a larger population have to be weighed against the risks of under treating a significant number of patients. In this study we have used the slit skin smear as the gold standard. The disadvantage of using it is that though a smear positive patient must fall into the MB group, it is not always necessary that a smear negative patient should receive PB.MDT. [7] Earlier studies have also demonstrated that the sensitivity of the clinical classification ranged from 85% to 93% and the specificity from 39% to 88%. [4],[5],[6],[7],[8] Rao et al , have also demonstrated that even within the group of patients with 1-5 skin lesions, there exists wide heterogeneity. [13] A prospective study on the effectiveness and safety of WHO/MDT among a cohort of patients in Thailand has recently been published. When the authors used a purely clinical classification system (≥6 lesions = MB), they found that 12% of the "true" MB patients would be under-treated as PB. They defined MB as cases with clinically diagnosed LL, BL or BB features, or any other cases with a BI of 2+ or more at any site. Their percentage of "missed" (false-negative) MB cases is very similar to the 11% we have found. [14] Since smear examination is not a practical alternative in resource poor settings, another parameter is required to replace it. This new parameter should be easy to teach and carry out by paramedical workers even in remote areas. In our study we have used the slit skin smear as a gold standard to measure the efficacy of using involved nerves in addition to skin lesions. The sensitivity rose to 94.4% when nerve examination alone was used. In actual terms, out of the 150 patients registered in this study, only two patients would have ended up being wrongly classified using this system. When skin and nerve examination are used together, the error rate falls to acceptable levels. Nerve examination is a tool that has been employed for decades in the examination of leprosy patients. It can be easily taught and mastered with continued use. Thus it seems to be an effective alternative to the slit skin smear in order to classify leprosy patients for the purpose of treatment. This can even be used in remote centers and in resource poor settings, as it does not require any laboratory equipment or trained technicians. th The WHO system of classifying leprosy cases as MB and PB is simple to apply and has a reasonable balance between sensitivity and specificity. However, it must be recognized that the system will lead to a small but significant number of skin-smear-positive MB cases being treated with a PB regimen. The addition of counting of nerve lesions can significantly improve the diagnostic efficacy. This system of classification and diagnosis based on clinical findings is simpler, more accurate and can be used even in resource poor settings. Acknowledgements The authors thank the medical superintendent of TLM Hospital, Shahdara, Dr. Laxmi Rajan for her kind cooperation.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08150t3.jpg] [dv08150t2.jpg] [dv08150t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}