 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
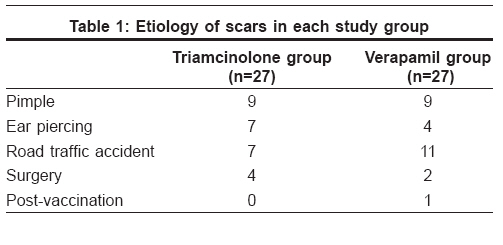
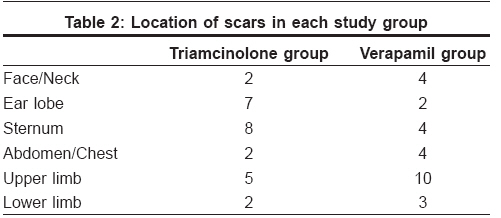
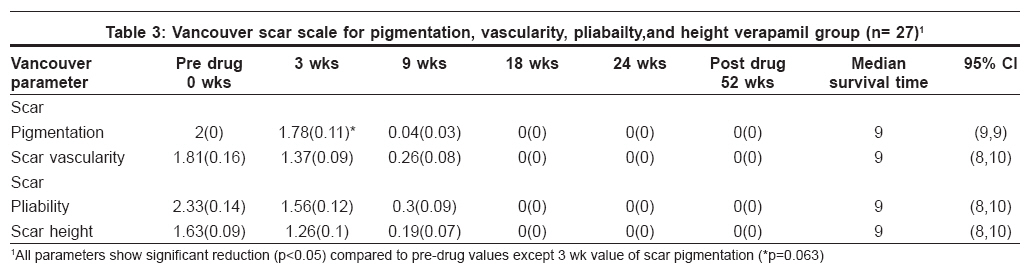
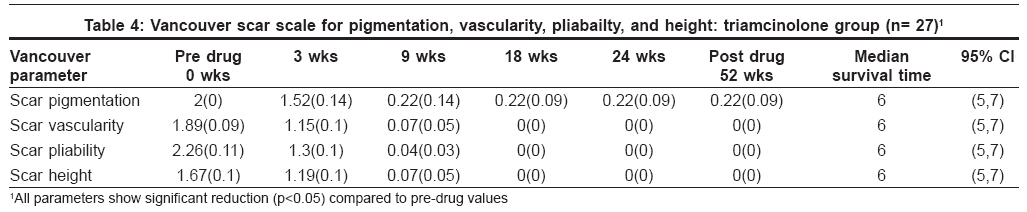
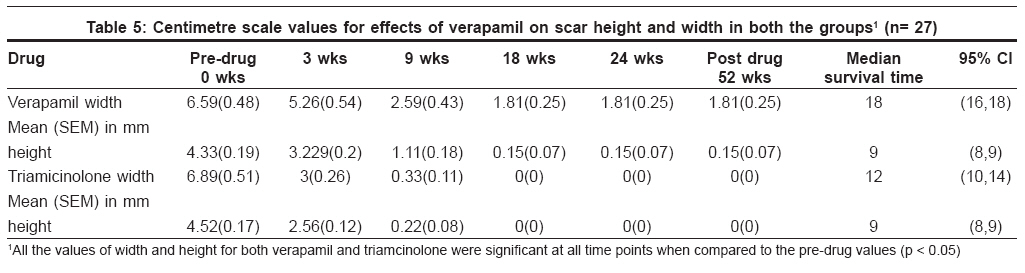
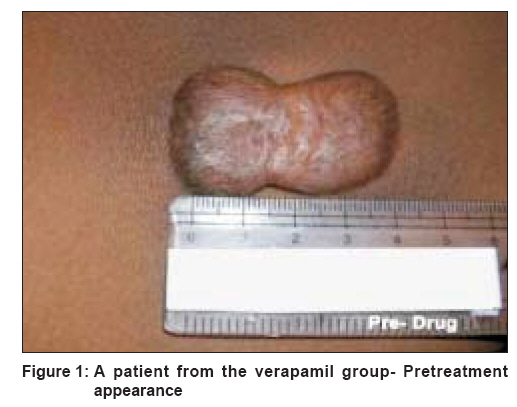
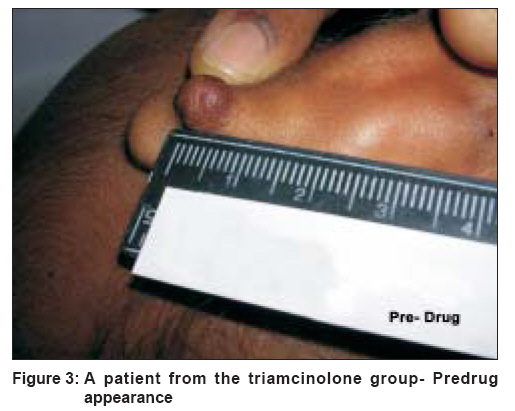
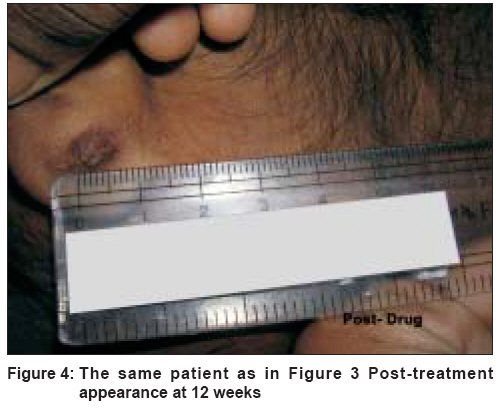
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 343-348 Original Article Comparison of intralesional verapamil with intralesional triamcinolone in the treatment of hypertrophic scars and keloids Margaret Shanthi FX, Ernest Kalpana, Dhanraj Prema Department of Pharmacology and Clinical Pharmacology, Christian Medical College, Vellore Code Number: dv08153 Abstract Background : The calcium channel blocker, verapamil stimulates procollagenase synthesis in keloids and hypertrophic scars.Aim : To study the effect of verapamil in the treatment of hypertrophic scars and keloids and to evaluate the effect of verapamil on the rate of reduction of hypertrophic scars and keloids in comparison with triamcinolone. Methods : The study was a randomized, single blind, parallel group study in which 54 patients were allocated to to receive either verapamil or triamcinolone. Drugs were administered intralesionally in both groups. Improvement of the scar was measured using modified Vancouver scale and by using a centimeter scale serially till the scar flattened. Results : There was a reduction in vascularity, pliability, height and width of the scar with both the drugs after 3 weeks of treatment. These changes were present at one year of follow-up after stopping treatment. Scar pigmentation was not changed desirably by either drug. Length of the scars was also not altered significantly by either drug. The rate of reduction in vascularity, pliability, height and width of the scar with triamcinolone was faster than with verapamil. Adverse drug reactions were more with triamcinolone than with verapamil. Conclusion : Intralesional verapamil may be a suitable alternative to triamcinolone in the treatment of hypertrophic scars and keloids. Keywords: Hypertrophic scar, Keloid, Triamcinolone, Verapamil Introduction Hypertrophic scars and keloids are dermal fibroproliferative disorders unique to humans that occur following trauma, inflammation, surgery, and that sometimes occur spontaneously. [1] They are characterized by excess development of collagen in the dermis and subcutaneous tissues. Unlike scar characteristics of normal wound repair, the exuberant scarring of keloid and hypertrophic scars can result in disfigurement, contractures, pruritus and pain. These cutaneous fibrotic conditions can be caused by minor trauma to the skin, such as ear piercing, abrasion, tattooing and burns. [2] Control of hypertrophic scars and keloids is a difficult challenge in surgical practice. [3] Currently there are several approaches for treating these conditions. The most common is application of compression bandages for 6 to 12 months. [4] Collagen and mucopolysaccharide creams, [5] radiotherapy, [6] laser therapy, [7] interferon therapy, [8] bleomycin [9] and intralesional corticosteroids are also used in the treatment and prophylaxis of hypertrophic scars and keloids. [10] The most commonly used corticosteroid is triamcinolone acetonide (TAC) at a concentration of 10-40 mg/ml, 1ml of which is administered intralesionally. Corticosteroids act by suppressing inflammatory cell migration, and inhibition of fibroblast proliferation at high doses. The calcium channel blocker verapamil has been shown to stimulate procollagenase synthesis in keloids, hypertrophic scars and normal human cultured fibroblasts, resulting in depolymerization of actin filaments, alteration of cell shape and reduction of fibrous tissue production. This study was hence conducted to assess the efficacy of intralesional verapamil in keloids and hypertrophic scars with regard to appearance, symptomatic improvement, patient satisfaction and complications by comparing it with the effects of intralesional triamcinolone. Methods The study used a randomized, single blind, parallel design to compare the effect of verapamil with that of triamcinolone on the healing of hypertrophic scars and keloids in two groups comprising 27 patients each. Patients who satisfied the selection criteria and gave written informed consent to participate in the study were chosen for the study. Inclusion criteria for the study were age of patients between 10 and 50 years; at least one hypertrophic scar or keloid; size of scar more than 2 to 10 cm and of less than 5 years duration; cause of scar being acid burns, trauma or surgery; insect bite or acne. The exclusion criteria used for the study were family history of keloids; dark pigmented skin, pregnancy or lactation; patients with systemic illness like diabetes mellitus, mental disorder, cancer and cardiac disease; and patients residing outside Vellore District, Tamil Nadu. Patients were randomly allocated using random numbers (Ralloc Soft Ware) to receive intralesional injection of 1ml of either verapamil (2.5 mg) or triamcinolone (40mg) every 3 weeks. Clinical assessment of the scars was performed at the beginning of the study and at 3 week intervals after starting treatment. The drugs were administered till the scar flattened or for a maximum period of 6 months. The patients were asked to return for scar examination after 1 year to check for any recurrence or complication The clinical assessment of the scar was based on the Vancouver Scar Scale which is the standard scale used universally for scar assessment. [11] This scale was slightly modified for Indian patients. The scale scores the scars on four parameters namely pigmentation, vascularity, pliability and height. In addition, the scar length, width and height also were measured using a centimeter scale. At each visit the patients′ scars were photographed on a digital camera Nikon ® Coolpix 3200. This study was conducted in the Outpatient Department of Plastic and Reconstructive Surgery, Christian Medical College, Vellore. The study was approved by the Institutional Ethics Committee. The sample size for the study was calculated to be 27 in each group on the basis of an alpha error of 0.05% (power of the study was 80%). For each study parameter in either group the mean value and standard error of mean (SEM) were calculated. The Wilcoxon Signed Rank Test was used for all statistical analyses. Kaplan Meier graphs and log rank test were done to compare the rate at which all the study parameters reduced to zero (zero is considered as the event), with the two drugs. A P value of less than 0.05 was considered to be statistically significant. Results Seventy two patients fulfilled the selection criteria of the study and were included in the study. Of the 72 patients, 38 subjects were allotted to the triamcinolone group and 34 to the verapamil group. Of these 54 (27 in each study group) were available for analysis after 12 months of the study. Seven in the verapamil group and 11 in the triamcinolone group were lost to follow up. The demographic details of the two study groups were as follows: the mean age of the patients in the verapamil group was 26 years and that in the triamcinolone group was 20 years. The male and female ratio in both study groups was the same. The etiology of scars of patients in each study group is shown in [Table - 1]. The location of scars of patients in each group is shown in [Table - 2]. For the Vancouver scale parameters, in both study groups there was a reduction in vascularity, pliability and height every third week. This reduction was maintained at 52 weeks in each study group as shown in [Table - 3] and [Table - 4]. A desired change in pigmentation was not seen with either of the two drugs. In fact, with triamcinolone, hyperpigmentation or hypopigmentation were noticed in 25% of patients. There was reduction in width and height of the scar every 3 weeks in both groups. Length of the scar did not show any significant change in both the groups as shown in [Table - 5]. The median time taken for reduction of all the parameters to zero was compared between the two drugs using Kaplan-Meier graphs and log rank tests. While comparing the median time taken for pigmentation to reduce to zero, there was no significant difference between the two drugs. The efficacy was assessed by the Vancouver scale parameters. The median time taken for reduction to zero in vascularity, pliability and height with triamcinolone was less as compared to verapamil and the difference was statistically significant. The median time taken for reduction to zero in length is not significant in either group. The median time taken for reduction to zero in width and height as measured with triamcinolone was less as compared to verapamil and the difference was statistically significant. Adverse drug reactions were experienced by patients in both study groups .Hypopigmentation , irregular menstrual cycles and profuse sweating were complications observed with triamcinolone. [Figure - 1] and [Figure - 2] represent one patients′ photographs in the verapamil group and [Figure - 3] and [Figure - 4] represent one patient′s photograph in the triamcinolone group. Discussion Hypertrophic scars and keloids are relatively common and important problems encountered in clinical practice. Despite many advances in the understanding of wound healing and scar formation, the treatment of these conditions is still controversial. [12] There are several nonpharmacological methods of treating hypertrophic scars and keloids but they have drawbacks like high cost (silicone gel sheeting), poor efficacy (surgery and laser therapy), recurrence (surgery) and adverse effects like malignancy (radiation therapy). Pharmacological modes of treatment also have drawbacks like poor efficacy (tacrolimus), high cost (bleomycin and interferon), recurrence (5-fluorouracil) and adverse drug reactions (5 - fluorouracil, bleomycin, interferon and triamcinolone). The prophylaxis of hypertrophic scar and keloid formation is more effective than its subsequent treatment. Prophylaxis involves the application of measures that reduce the risk of the development of problem-causing scars. The pathogenesis of keloids includes excessive amount of collagen and other extracellular matrix components. Abergel et al , [13] showed an abnormal composition and metabolism of collagen in hypertrophic scars and keloids. Calcium channel blockers were first used in collagen matrix on the connective tissue remodeling by Lee and Ping in 1990 [14] who suggested that they depolymerize actin filaments and alter the shape of fibroblast cells from bipolar to spherical and that this process results in an increase in procollagenase production. The first successful results of the intralesional injection of verapamil were presented in 1994 in burns scars. [15] Lawrence, [16] presented his experience with the intralesional verapamil injection and pressure therapy in the treatment of earlobe scars and reported a cure rate of 50%. D′Andrea et al , [17] suggested that the treatment of keloids with perilesional surgical excision and topical silicone followed by an adjuvant treatment with intralesional verapamil hydrochloride injection at certain intervals offered a higher rate of resolution than other therapeutic strategies. The present study compared the efficacy of intralesional verapamil with that of intralesional triamcinolone in the treatment of hypertrophic scars and keloids using a randomized, single-blind study design. It was not possible to use a double-blind study design in the present study because triamcinolone is an oily emulsion whereas verapamil is a plain coloured solution. The many methods for following the progress or maturation of a scar include scar elastometry, negative imaging, photography, biopsy and clinical evaluation. [18] High resolution ultrasonic scanning is also used. [19] Use of a non- contact 3D digitizer to measure the volume of keloid scars is also used. [20] Hypertrophic scars were not distinguished from keloid scars using electron microscopy in the present study due to financial constraints. Electron microscopy would have given confirmative evidence of the differences between hypertrophic scars and keloids. It was found in the present study that intralesionally administered verapamil and triamcinolone improved hypertrophic scars and keloids in the patients. Clinical parameters of the scar like vascularity, pliability and height shown in [Table - 3] and [Table - 4] (measured using Vancouver scale) and width and height shown in [Table - 5] (measured using centimeter scale) showed improvement. The improvement was noted after 3 weeks of treatment with both triamcinolone and verapamil and was present after one year of follow-up after stopping treatment. Scar pigmentation was not changed desirably by either drug. With triamcinolone, hypopigmentation or hyperpigmentation were noticed in some of the patients. Length of the scars was not altered significantly by both the drugs. To our knowledge this is the first randomized controlled study to demonstrate the efficacy of intralesional verapamil in the treatment of hypertrophic scars and keloids. There have been other reports showing the efficacy of intralesional verapamil in the treatment of these disorders, but they have been case reports or studies that used surgical treatment in conjunction with verapamil. The results of the present study suggest that verapamil is clinically safe for patients with hypertrophic scars and keloids. When compared with other methods of treatment, injection of verapamil appears to be capable of inducing a rapid beneficial effect in the scars. Verapamil, in addition to being effective in treating hypertrophic scars and keloids in the present study, was also found to be less toxic than triamcinolone, causing a lower incidence of adverse drug reactions. Other advantages of verapamil over triamcinolone include the considerably lower cost of verapamil than triamcinolone, which has implications for developing countries like India. Moreover, verapamil, being a solution, is much easier to inject intralesionally than triamcinolone which is an oily emulsion causing severe pain at the injection site. In conclusion, the present study compared the efficacy of verapamil with that of triamcinolone in treating hypertrophic scars and keloids, both drugs given by injection intralesionally. It was found that verapamil, like triamcinolone, significantly improved all clinical parameters of the scars that were investigated. The improvement was observed after 3 weeks of treatment and was present one year after follow-up. Patient acceptability of verapamil was also found to be good and the incidence of adverse drug reactions was found to be lower in patients who received verapamil than in those who received triamcinolone. Hence, intralesional verapamil may be a suitable alternative to triamcinolone in the treatment of hypertrophic scars and keloids. Acknowledgements We thank CMC Fluid Research Grant committee for funding this project. We express our heart felt gratitude to Dr. Jacob Peedicayil, Professor of Pharmacology, Christian Medical College, Vellore for his inspiring guidance, supervision and continuous encouragement at every step of the project work.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08153t1.jpg] [dv08153f3.jpg] [dv08153t4.jpg] [dv08153t2.jpg] [dv08153t3.jpg] [dv08153t5.jpg] [dv08153f1.jpg] [dv08153f2.jpg] [dv08153f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}