 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
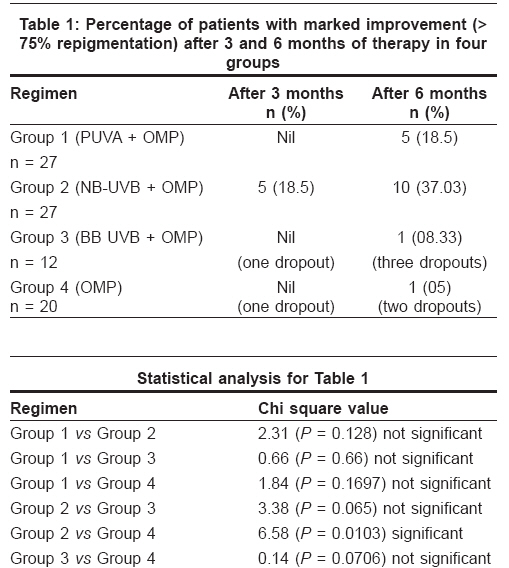
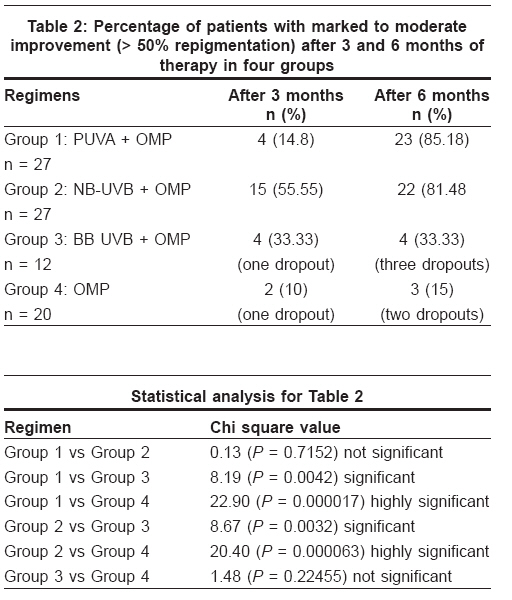
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 357-360 Brief Report An open labeled, comparative clinical study on efficacy and tolerability of oral minipulse of steroid (OMP) alone, OMP with PUVA and broad / narrow band UVB phototherapy in progressive vitiligo Rath Namita, Kar HK, Sabhnani Sunil Department of Dermatology and STD, Dr. RML Hospital, New Delhi Code Number: dv08156 Abstract Background: Several modalities of treatment have been tried in vitiligo with varied results; however, Indian data on comparative studies of two or more therapies are limited.Aims: We compared different phototherapy methods with an oral steroid as an adjunct to determine the method with the best tolerability and efficacy. Methods: Eighty-six patients with progressive vitiligo were randomly assigned to different study groups according to a continuous selection method over a period of one year. Group 1 was given OMP + PUVA, group 2 OMP + UVB (NB), group 3 OMP + UVB (BB) and group 4 was given OMP alone. Each patient was followed up for six months and then released from treatment. Clinical evaluation was made at the end of three and six months. Results: In group 1 (OMP + PUVA), marked improvement was seen in 18.51% while moderate improvement was seen in 66.66% of the patients. Marked improvement was seen in 37.03% in group 2 (OMP + NB-UVB) while 44.44% had moderate improvement. In group 3 (OMP + BB UVB), 8.33% showed marked improvement while moderate improvement was seen in 25% of the patients. Marked and moderate improvement was seen in 5 and 10% of group 4 (OMP) patients, respectively. Conclusions: Our study compared four treatment modalities in vitiligo patients, out of which oral minipulse of steroids (OMP) only had an adjunct value and was not very effective by itself. Narrow band UVB has a definite edge over broad band UVB and should be preferred when both options are available. NB-UVB and PUVA showed comparable efficacy. Keywords: Oral Minipulse, PUVA, Narrow Band (UVB), Broad Band UVB, Vitiligo Introduction Vitiligo is a common idiopathic disorder characterized clinically by white macules on the skin. [1] Several modalities of treatment have been tried with varied results; however, Indian data on comparative studies of two or more therapies are limited. Phototherapy is quite effective, and while many patients may not experience complete repigmentation, 50-75% repigmentation can be routinely expected in vitiligo of recent onset. [2] As many patients will achieve only partial repigmentation even with the best of therapies, therapies may be cycled or combined to achieve higher overall repigmentation rates and to minimize side effects of therapy. [3] The aims of vitiligo therapy are two-fold: to repigment and remit disease progression. We have carried out a comparative study of different phototherapy methods with oral steroids as adjunct to determine the method with the best tolerability and efficacy.Methods A total of 86 patients were included in the study. These patients were in the age group of 10-50 years and had progressive vitiligo involving 25-50% of the body surface area. Exclusion criteria were patients with diabetes and hypertension, > 50% body surface area involvement, and those with history of photosensitivity and photodermatitis. Patients were assigned to four study groups and all four groups received oral minipulses (OMP) of betamethasone, 0.1 mg/kg body weight twice weekly on two consecutive days for three months followed by tapering of the dose by 1 mg every month over the following three months. Group 1 consisted of 27 patients, all of whom received OMP as described above, along with psoralen with ultraviolet A light (PUVA) therapy in the form of 8-methoxypsoralen 0.6 mg/kg on alternate days plus UVA 320-400 nm from a Waldman W UV-7001 K phototherapy whole body chamber having both UVA and UVB (BB) tubes. The initial dose was 0.5 J/cm 2 UVA with increments of 0.2 J/cm 2 for every third dose (up to a maximum of 6 J/cm 2 ). Group 2 also consisted of 27 patients who, in addition to OMP, received narrow band UVB (NB-UVB). The initial dose was 0.3 J/cm 2 with increments of 0.1 J/cm 2 in every dose (up to a maximum of 3 J/cm 2 ) using a Waldmann W UV 1000 L whole body phototherapy chamber containing NB-UVB (Phillips TL01) tubes. Doses were given thrice weekly in order to maintain an optimal constant dose with minimal erythema. Group 3 consisted of 12 patients who were given OMP and broad band UVB (290-320 nm) on alternate days using the same chamber used for Group 1. Initial dose was 0.05 J/cm 2 with increments of 0.02 J/cm 2 for every third dose. Phototherapy was given thrice weekly and efforts were made to maintain an optimal constant dose with minimal erythema. There were fewer patients in this group because no new patients were assigned due to the excessive erythema observed in six patients. Group 4 consisted of 20 patients who were given only OMP. Patients were randomly assigned to different study groups according to a continuous selection method over a period of one year. Each patient was treated for six months and then released from the above scheduled treatment regimens. Clinical evaluation was made at the end of three and six months. Improvement was categorized as marked (> 75% repigmentation), moderate (50-75% repigmentation), mild (25-50% repigmentation) and poor or no (< 25% repigmentation) improvement. Side effects were noted in every case. Results At the end of three months , there was moderate improvement in four (14.8%) patients in group 1 (OMP + PUVA) while mild improvement was seen in 11 (40%) patients; the remaining twelve patients showed < 25% improvement. In group 2 (OMP + NB-UVB) patients, there was marked improvement in five (18.51%) patients and moderate improvement in ten (37.03%) patients [Table - 1]. Mild improvement was seen in 11 (40.74%) patients while one patient showed < 25% improvement. Moderate improvement was seen in four group 3 (OMP+BB UVB) patients (33.33%) and mild improvement in three patients (25%). Four patients had < 25% improvement whereas one patient dropped out of the study. In group 4 (OMP alone), moderate improvement was seen in two patients (10%) and mild improvement in 17 patients (85%); one patient dropped out of the study. At the end of six months, marked improvement was seen in five group 1 (OMP + PUVA) patients (18.51%) while moderate and mild improvement was seen in 18 (66.66%) and four (14.8%) patients respectively. In this group, side effects such as nausea and weight gain (Cushingoid habitus) were experienced by 11 patients (40.74%) and excessive erythema and blistering were observed in five patients (18.51%) in whom one to three doses were skipped and treatment later resumed with a reduced dose. Roughness of the skin was present in 20 patients (74.07%); all patients had perilesional hyperpigmentation. Marked improvement was seen in ten patients (37.03%) in group 2 (OMP + NB-UVB). Twelve patients (44.44%) had moderate improvement, while five patients (18.51%) showed mild improvement. All patients (100%) were tanned, while weight gain was experienced by ten patients (37.03%). In group 3 (OMP + BB UVB), only one patient (8.33%) showed marked improvement, while moderate and mild improvement was seen in three (25%) and five patients (41.66%) respectively. Three patients dropped out of the study because of side effects that included excessive erythema in six patients (50%) and weight gain in five patients (41.66%). Out of 20 group-4 (OMP alone) patients, marked improvement was seen in only one patient (5%). Moderate and mild improvement occurred in two (10%) and 15 (75%) patients (10%) respectively. Two patients dropped out due to weight gain and ten patients (50%) experienced weight gain. Group-2 patients demonstrated more marked improvement than other patients. The Chi Square test was applied with the help of SPSS-12 and found that only the comparison between group-2 and group-4 was statistically significant at a 5% level of significance. More group-1 patients had marked to moderate improvement than other groups [Table - 2]. The Chi Square test was applied with the help of SPSS-12 and found that while the group-1 vs group-2 and group-3 vs group-4 comparisons were not significant at a 5% level of significance, the group 1 vs group 4 and group 2 vs group 4 comparisons were highly significant at 5% level of significance. Discussion Phototherapy using oral psoralens and UVA (320-400 nm) has been in use for a very long time. The ultraviolet A radiation (UVA) can be either from an artificial source or from natural sunlight (PUVASOL). [4] Narrow band UVB (NB-UVB) utilizes the effective UVB range and excludes erythema-inducing rays, thus having a definite edge over broad band UVB. The advantages of NB-UVB phototherapy are shorter sessions and suitability in children and pregnancy. No oral psoralens are required and there is no phototoxicity, xerosis, or hyperkeratosis as seen with PUVA. [5] The effect of NB-UVB was first highlighted in a study by Westerhof and Nieweboer-Krobotova in 1997. [6] They compared topical PUVA with NB-UVB and found that 67% of patients receiving narrow band UVB showed repigmentation after four months in comparison to 46% of cases receiving topical PUVA. In that 1997 study , 8% of the patients showed > 75% repigmentation after three months with NB-UVB. In our study, there was marked improvement in five (18.51%) patients and moderate improvement in ten (37.03%) patients after three months of administering narrowband UVB along with OMP. The mechanism of pigmentation following UVB radiation is still unknown. It has been suggested that endothelin and tyrosinase expressed by keratinocytes may play a role in the resulting pigmentation. [7] Njoo, Bos and Westerhof carried out an open study with narrow band UVB in 51 children with generalized vitiligo for one year. They reported > 75% repigmentation in 53% of their patients. [8] More than 75% repigmentation was also reported in a recent study by Kanwar et al , who followed up 26 children with generalized vitiligo receiving narrow band UVB. [9] Njoo et al , did a meta-analysis of nonsurgical pigmentation therapies in vitiligo. They found that repigmentation occurred in 51% of patients on oral PUVA, in 57% of those on BB UVB and in 63% of patients on narrow band UVB. [10] In our study after three months, > 50% of the patients receiving narrow band UVB showed marked and moderate improvement while only 14.8% showed moderate improvement with PUVA (both having OMP as an adjunct). After six months, we found that > 85% patients of patients undergoing PUVA treatment showed moderate to marked improvement while > 81% of those receiving narrow band UVB showed moderate to marked improvement. This highlighted the fact that although narrow band UVB causes faster repigmentation, both PUVA and narrowband UVB have comparable effects over time. Pasricha and Khaitan tried oral minipulses of betamethasone in 1993. They reported 26-50% repigmentation in 25% of their patients, 51-75% repigmentation in 7.5% and > 75% repigmentation in 15% of the patients. [11] In our study, we gave twenty patients oral minipulses (OMP) and marked improvement was seen in only one patient (5%). Moderate improvement occurred in two patients (10%) while mild improvement was seen in 15 patients (75%). In contrast, > 75% improvement was seen in group 2 (NB-UVB + OMP) patients, an observation that was statistically significant at a 5% level of significance when compared to group 4 (OMP) patients after three and six months. Statistical analysis of marked to moderate improvement (> 50% repigmentation) was done with the help of SPSS-12 using the Chi square test. It was found that only the Group 1 vs Group 2 and Group 3 vs Group 4 comparisons were not significant at a 5% level of significance. Group 1 vs Group 4 and Group 2 vs Group 4 comparisons were highly significant at a 5% level of significance. It was found that, out of the four treatment modalities , OMP has only an adjunct value and helps in the arrest of the disease progress, but has no significant, intrinsic repigmenting efficacy. Our patients experienced side effects such as tanning, erythema due to ultraviolet therapy and bloating, weight gain due to oral steroids-all of which were reported in earlier studies too. [8],[9],[11] This study is being reported for its uniqueness in that no study has been reported, to date, that compares these four modalities along with oral minipulses of steroids. However, an extensive study with a larger population and longer follow-up period is warranted for more conclusive evidence. Acknowledgements Financial and material support for this study was provided by Pool Section, Human Resource Development (HRD) group, Council of Scientific and Industrial Research (CSIR), Pusa, New Delhi.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08156t2.jpg] [dv08156t1.jpg] |
| |||||||||

{kind=link}
{kind=link}