 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
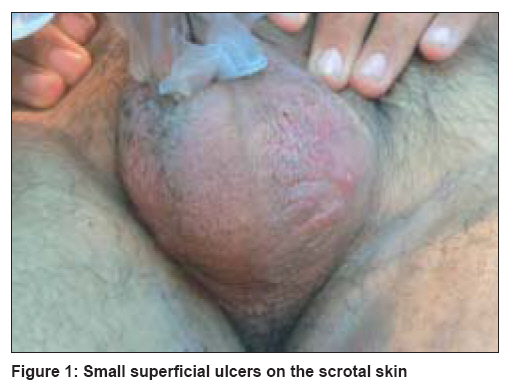
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 383-384 Letter To Editor Chikungunya-induced genital ulcers Mishra Katyayan, Rajawat Vishwesh Consultant Dermatologist, Ujjain (Madhya Pradesh) Code Number: dv08163 Sir, Chikungunya fever, which is caused by a togavirus (arboviral infection), manifests as an acute illness of fever, headache, arthralgia, vomiting, abdominal pain, sore throat, conjunctivitis and lymphadenopathy. [1] The chikungunya virus was first isolated from patients and Aedes aegypti mosquitoes from Tanzania in 1952. The virus first appeared in India in 1963 when along with dengue, it caused very extensive epidemics in Calcutta, Madras and other areas. This current outbreak had started in June-July in 2006. It presents as a fever of sudden onset, crippling joint pains, lymphadenopathy and conjunctivitis. A total of 60098 suspected cases were reported, out of which 70 cases were confirmed by serum ELISA test. [2] A maculopapular rash [3] is common and some cases even show hemorrhagic manifestations, [4] which have not been reported after 1973. The fever is typically biphasic with a period of remission of 1-6 days. No vaccine is available. Various outbreaks have been reported from Asia, East Africa and peninsular India. The incubation period is 2-4 days and the illness is self-limiting with two phases of fever lasting for about 3-10 days. Very few reports of dermatological manifestations exist. [5],[6] During the recent epidemic of chikungunya fever in central India, we encountered 16 young adult males with penoscrotal ulcerations. All patients were in the age group of 20-45 years, and had developed these ulcers after about 13-35 days of developing fever, clinically thought to be chikungunya. Apart from the fever with chills, they had headache, nausea, vomiting and joint pains. The skin lesions were punched-out, deep ulcers with undermined edges showing healthy granulation tissue in the floor but erythema and thickening in the surrounding skin [Figure - 1]. The size of the ulcers varied from 0.5-2 cm in diameter and their shape was round to oval or irregular. The number of ulcers per patient ranged from 1-3. These patients were from a rural background and were clinically diagnosed as Chikungunya. However, no viral isolation or culture was performed in these cases as the facilities to perform these techniques were unavailable in rural India. Blood counts were normal in all the cases. Bacterial cultures of the material from the ulcers were performed in three cases and did not grow any organisms after 72 hours of inoculation. Biopsy from the edge of the ulcer was performed in one case and showed dermal edema and perivascular, mononuclear infiltrate as the prominent features. We treated the ulcers with oral erythromycin 500 mg QID and prednisolone 0.5 mg/kg per day for 7-10 days and all of them healed with scarring within 10-26 days. The word "chikungunya" is derived from the description in Swahili of the contorted posture of patients afflicted with the severe joint pain associated with this disease. [6] Additional dermatological manifestations reported in recent outbreaks of Chikungunya fever in Southern India include nasal erythema, freckle-like pigmentation over the centro-facial area, lichenoid eruption and hyperpigmentation in sun-exposed areas, lymphedema in acral distribution, multiple ecchymotic spots, vesico-bullous lesions and urticaria. [6] These types of cutaneous ulcers at the peno-scrotal junction and on the scrotum have never been reported in published literature before. However, similar findings were reported unpublished observations from India. [5] We believe that clinicians should be aware of this picture, as these lesions are self-limiting and usually heal with antibiotics and oral steroids. Although none of the patients discussed here were tested for the arboviral infection, the clinical picture of fever and joint pain was very typical of chikungunya. Although most of these patients had received non-steroidal anti-inflammatory drugs (NSAIDs) for joint pains these ulcers did not appear to be drug-induced fixed drug eruption or Stevens Johnson syndrome. The peno-scrotal ulcers probably represent a reaction pattern in this type of viral illness which has, to the best of our knowledge, never been published in literature. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08163f1.jpg] |
| |||||||||

{kind=link}