 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
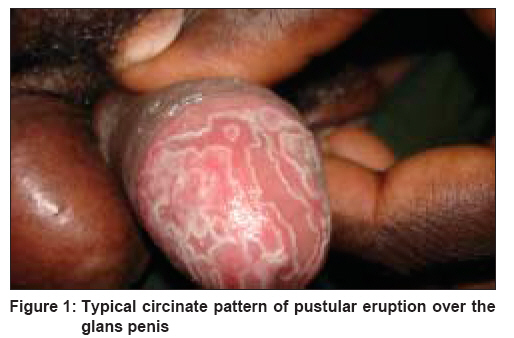
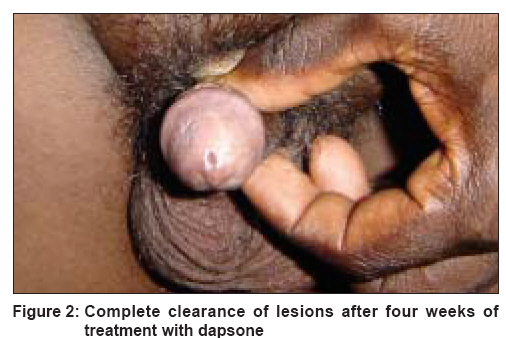
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 388-389 Letter To Editor Circinate pustular psoriasis localized to glans penis mimicking 'circinate balanitis' and responsive to dapsone Singh Nidhi, Thappa DevinderMohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: dv08167 Sir, Pustular psoriasis is of two major types: localized and generalized. [1] Localized pustular psoriasis is usually confined to the hands and feet and tends to be chronic. Generalized pustular psoriasis may involve the whole body, having a subacute, acute or even fulminating and life-threatening course. [2] Annular pustular psoriasis which is usually generalized, is also reported as being localized to the dorsa of the feet. [3] Although localized pustular psoriasis usually presents over the hands and feet, only one case report has been reported of localized pustular psoriasis involving the penis. [4] We herein report a case of circinate pustular psoriasis over the glans penis mimicking circinate balanitis. A 37 year-old married man presented with recurrent episodes of multiple, painless, pustular eruptions over the glans penis of four years′ duration. He gave no history of fever, joint pains, redness or burning sensation of the eyes or skin or mucosal lesions elsewhere in his body. Treatment with antibiotics (doxycycline, metronidazole, and penicillin) and topical steroid ointments resulted in remissions. Local examination revealed a typical circinate pattern of pustular eruption over the glans penis. These lesions morphologically mimicked circinate balanitis [Figure - 1]; systemic examination was unremarkable. Ophthalmological examination was normal. Darkfield microscopy was negative and so were KOH scrapings for candida. Serology for syphilis [Venereal disease research laboratory test (VDRL) and treponema pallidum hemagglutination test (TPHA) and HIV (ELISA)] was negative; routine urine microscopy was not rewarding. Histopathological examination of the lesion over the glans penis revealed mild hyperkeratosis and neutrophilic aggregations in the superficial layer of epidermis. There were marked dysplastic changes in the epidermis and a chronic lymphocytic infiltrate in the upper dermis. These features were compatible with pustular psoriasis. The patient was treated with dapsone 100 mg daily. The glans lesions subsided completely in four weeks [Figure - 2]. Subsequently, the patient was put on maintenance therapy with dapsone 50 mg daily. Circinate, annular and other patterned lesions may be seen in acute generalized pustular psoriasis, but are more characteristic of subacute or chronic forms of widespread pustular psoriasis. [2] These lesions begin as discrete areas of erythema following exfoliation of the pustules-pustules appear peripherally on the crest of the advancing edge, become desiccated and leave a trailing fringe of scale as the lesion slowly advances. Lapiere [5] had described a recurrent circinate erythematous psoriasis that may occur alone in complete absence of any stage of psoriasis, or may occur as a part of generalized pustular psoriasis. Linear forms of pustular psoriasis may occasionally be observed within the context of a more generalized psoriasis. [2] Differential diagnosis of our case included circinate balanitis of Reiter′s disease and pustular secondary syphilis. Reiter′s disease was excluded on the basis of the absence of peripheral arthritis, urethritis and conjunctivitis. [6] Pustular secondary syphilis was ruled out due to the absence of skin lesions elsewhere, negative darkfield microscopy and serology. [7] Recurrent clinical pustular course and the circinate pattern in the absence of the features of Reiter′s disease, and the typical histopathology helped us to arrive at the diagnosis of localized pustular psoriasis of the glans penis. Usually the circinate variant of pustular psoriasis is generalized, but in our case it was localized to the glans penis. A case of pustular psoriasis limited to the penis has been documented in the literature. [4] Localized pustular psoriasis is usually refractory to treatment. [3] Treatments include the use of topical steroids, tar preparation and systemic therapy with etretinate and PUVA (psoralen with ultraviolet A). [3] However, aggressive topical and phototherapeutic treatment modalities can lead to worsening of the condition. [8] Tetracycline, cyclosporine, and methotrexate have been found to be effective. [2] Dapsone and clofazimine have been found to be effective in anectodal reports; [2] our patient showed a dramatic response to dapsone. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08167f2.jpg] [dv08167f1.jpg] |
| |||||||||

{kind=link}
{kind=link}