 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
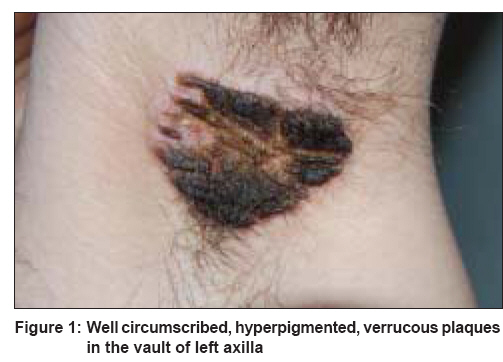
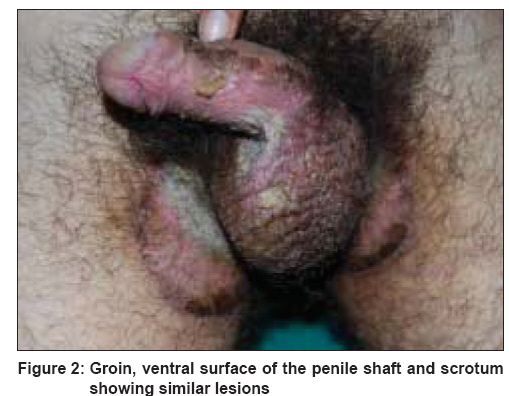
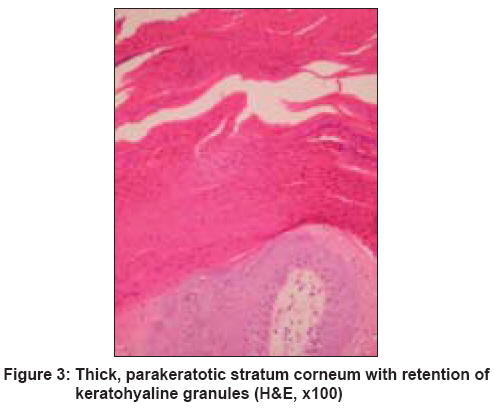
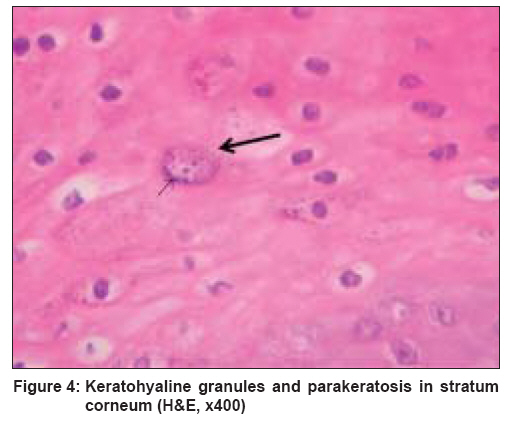
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 405-407 Letter To Editor Intertriginous granular parakeratosis persisting for 20 years Reddy IS, Swarnalata G, Mody Tejal Department of Dermatology, Apollo Hospitals, Jubilee Hills, Hyderabad 500 033 Code Number: dv08181 Sir, We read with interest the article "Granular parakeratosis presenting with facial keratotic papules" by Joshi and Taneja. [1] We report here a case of granular parakeratosis that involves multiple intertriginous areas. A 25 year-old male presented with a pruritic eruption in the flexures that had been prevalent since he was five years old. The eruption was persistent throughout this period except for brief intervening periods, during which it resolved completely when he lived in cooler climatic conditions. He denied the use of deodorants, antiperspirants, and body sprays. No other family member had similar skin lesions. Examination revealed multiple, hyperpigmented, linear, verrucous papules coalescing to form well-delineated, annular plaques in the vault of the axillae [Figure - 1]. A well-defined, semiannular, hyperpigmented, macerated plaque was seen along with erosions and crusting over the groin, ventral surface of the penile shaft and the glans penis [Figure - 2]. A well-defined, moist, macerated, grayish-white plaque was present between the buttocks and the perianal region. The clinical differential diagnoses considered were Hailey-Hailey disease and pemphigus vegetans. A potassium hydroxide wet mount preparation from the lesion did not show any fungal hyphae. Skin biopsy showed a markedly thickened and compact stratum corneum. The nuclei were preserved throughout the thickened stratum corneum [Figure - 3]. Instead of the expected absence of keratohyaline granules from the cytoplasm of horny cells, these organelles were present throughout the stratum corneum [Figure - 4]. A thickened stratum granulosum was observed. There was no evidence of neutrophils in the epidermis. Spongiosis and acantholysis were absent and direct immunofluorescence did not show any immune deposits in the epidermis. Correlating the distribution and morphology of the lesions with the histology, a diagnosis of intertriginous granular parakerotosis was made. The patient did not respond to topical steroids, antibiotics, antifungals, tretinoin or oral isotretinoin. In 1991, Northcutt, Nelson, and Tschen described a clinicopathological entity from a series of biopsy specimens of axillary lesions that showed an unusual and unique form of parakeratosis which they designated as "axillary granular parakeratosis". [2] In 1998, Mehregan, Thomas, and Mehregan described four more cases of granular parakeratosis, including a patient with isolated involvement of the inguinal region and suggested that the term "axillary granular parakeratosis" may be re-designated as "intertriginous granular parakeratosis." [3] Although more common in middle-aged and elderly women, granular parakeratosis can occur in both sexes and in all age groups. It has been described in infants as linear and geometric scaly plaques over the pressure points beneath their diapers. [4] Rarely, as reported by Joshi and Taneja, it can also occur over non-intertriginous areas such as the face. [1] Contact allergens and physical factors such as heat, moisture, friction, obesity, and occlusion from diapers were suspected to play a role. The resolution of the lesions in cooler climates points to sweating and friction as two possible factors responsible for the parakeratosis seen in our case. It is presumed that granular parakeratosis is a reaction pattern secondary to various stimuli rather than a distinctive disease. [5] The disturbance in keratinization in the form of a blockade of the conversion of profilaggrin into filaggrin units is suspected to be a basic pathogenic abnormality. Other than the characteristic distribution of lesions and unique histopathological features, granular parakeratosis has been observed as an incidental histopathologic finding in various unrelated conditions such as dermatomyositis, dermatophytosis, and molluscum contagiosum. The therapeutic response of granular parakeratosis to various modalities of treatment has been inconsistent and frequently disappointing, and no controlled therapeutic trials have been conducted. Individual case reports have shown response to topical tretinoin [6] and to isotretinoin. [7] There are reports in which these eruptions responded to topically applied glucocorticoids, [8] antifungals, and antibiotics, as well as reports which showed no response to the above medications. A review of literature confirmed that prevalence of these eruptions for 20 years (as observed in our patient) is the longest of all such reported cases. Involvement of multiple intertriginous areas has been published earlier, [9] and this patient is the second such case to be reported. To conclude, this case is presented for its rarity, extreme chronicity, and the involvement of multiple intertriginous areas. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08181f2.jpg] [dv08181f1.jpg] [dv08181f4.jpg] [dv08181f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}