 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
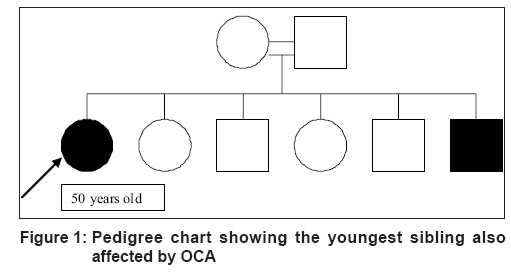
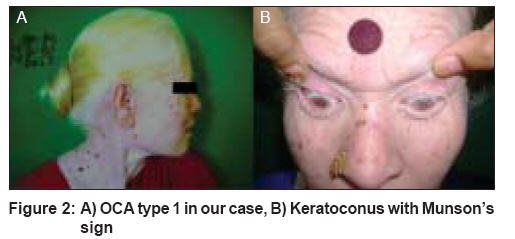
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 407-409 Letter To Editor Bilateral keratoconus with oculocutaneous albinism Rao VasudevAnand, Swathi P, Chaitra, Thappa DevinderMohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: dv08182 Sir, Keratoconus (KC) is a progressive, non-inflammatory, bilateral, usually asymmetrical disease of the cornea, characterized by paraxial, stromal thinning that leads to corneal surface distortion. Visual disturbance occurs primarily from irregular astigmatism and myopia, and secondarily from corneal scarring leading to a mild to marked impairment in the quality of life. [1] Albinism, a genetically determined heterogeneous group of disorders involving hypopigmentation of the skin, eyes, hair (oculocutaneous albinism) or the eyes alone (ocular albinism), occurs primarily due to a deficiency of tyrosinase, which mediates the conversion of tyrosine to melanin. [2] Keratoconus is commonly an isolated condition despite multiple singular reports of its coexistence with other disorders. [1] We report here a case of bilateral keratoconus in oculocutaneous albinism which, to the best of our knowledge, has not been reported so far in literature. A 50 year-old female, a known case of oculocutaneous albinism (OCA) type 1, presented to us with diminution of vision since her childhood with deterioration for the past four months. She had a history of frequent rubbing of her eyes and photophobia. She had a positive family history in which the last sibling was similarly affected [Figure - 1]. On physical examination, she was seen to have light skin and light blond hair with poliosis and heterochromia iridum. Her skin did not tan and her neck and nape areas showed signs of photodamage in the form of dermatoheliosis. On ophthalmological examination, both eyes were found to have visual acuity (she was able to see the number of fingers held close to her face) with accurate projection of rays, horizontal pendular nystagmus, and a positive Munson′s sign (tenting of the lower lid during a downward gaze) [Figure - 2]. On slit lamp examination, her cornea showed thinning with conical protrusion in both the eyes (the right more than the left). There was stromal scarring in the inferotemporal aspect, Fleisher′s ring (deposition of hemosiderin at the level of the Bowman′s membrane in the base of the cone) and Vogt′s striae (vertical tears in the Descemet′s membrane) in the right eye. In both eyes, the iris showed transillumination and the lens was cataractous. Extended keratometry was 60D in right eye and 52D in the left eye. The fundus could not be visualized in either eye due to dense cataracts. Cataract extraction for both eyes has been planned to manage the patient′s condition and penetrating keratoplasty will be considered at a later date for the right eye. Oculocutaneous albinism (OCA) is the most common inherited disorder of generalized hypopigmentation, with an estimated frequency of 1:20,000 in most populations. [2] The OCA1 (tyrosine-negative) and OCA2 (tyrosine-positive) are the most frequently observed types and account for approximately 40 and 50% respectively of OCA cases all over the world. OCA3 and 4 are far less frequent. [2] The inheritance pattern is autosomal recessive. OCA1 is the most severe form of albinism that occurs due to mutations in the tyrosinase [TYR] gene found on chromosome11q14-q21. In OCA 2, pheomelanin is produced due to mutations in the OCA2 gene localized to chromosome 15q11.2-q12. [2] Most common ocular changes seen in OCA are a reduction in the iris and retinal pigment, foveal hypoplasia, misrouting of optic fibres at the optic chiasma, nystagmus, and alternating strabismus. [3] A few other ocular changes that have been reported are Duane retraction syndrome, [3] corneal mesodermal dysgenesis, [4] and congenital glaucoma. [5] Keratoconus is a slowly progressive condition that often presents in the teenage years or in the early twenties, with decreased vision or visual distortion and a reported incidence of approximately 1 per 2000 in the general population. [1] It is rarely congenital. Commonly recognized associations are Down′s syndrome, Leber′s congenital amaurosis, and connective tissue disorders. Atopic dermatitis has been found to be commonly associated, a probable mechanism for keratoconus in this condition being the constant rubbing of eyes. Thus, our case is unique in that oculocutaneous albinism is associated with keratoconus, altthough this could be an incidental association. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08182f2.jpg] [dv08182f1.jpg] |
| |||||||||

{kind=link}
{kind=link}