 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
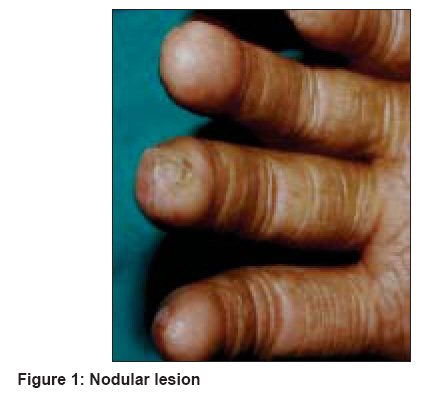
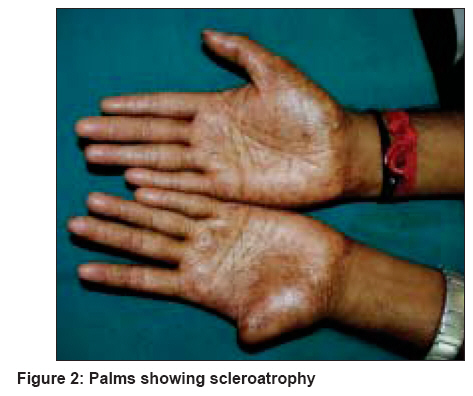
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 409-410 Letter To Editor Huriez syndrome Sekar ShanmugaC, Srinivas CR Department of Dermatology, PSG Hospitals, Peelamedu, Coimbatore Code Number: dv08183 Sir, Huriez syndrome is a rare autosomal dominant condition characterized by scleroatrophy of the palms and the soles, palmoplantar keratoderma, as well as nail changes. The development of squamous cell carcinoma in the scleroatrophic area is the most dreaded complication of this syndrome. Huriez syndrome also referred to as "sclerotylosis," is an autosomal dominant genodermatosis, characterized by the triad of congenital scleroatrophy of the distal extremities, palmoplantar keratoderma (PPK), and hypoplastic nail changes. It was first described in two large pedigrees from northern France. [1] The development of aggressive squamous cell carcinoma (SCC) of the affected skin is a distinctive feature of the syndrome, occurring in around 15% of affected individuals. SCC in Huriez syndrome is characterized by its early onset and metastasis. [2] The pathogenetic mechanism of tumorigenesis in Huriez syndrome is unknown. We report here the first case of Huriez syndrome from India. A 27 year-old male presented with a raised nodular lesion on the left middle finger that had been prevalent since four months [Figure - 1]. The lesion started as a small, warty papule and gradually increased in size. The patient had a similar lesion on the left thumb a year ago, which was excised and diagnosed as a squamous cell carcinoma. The left thumb had been amputated, the draining nodes removed, and chemotherapy given for six months. The patient had a history of dryness with pigmentation and recurrent fissuring of the palmar skin since his birth. He was a software engineer and had no exposure to chemicals or drugs that could cause sclerosis of the skin. There were no similar complaints in any of the family members. On examination, the palms were seen to have diffuse scleroatrophy with fissuring and hyperpigmentation [Figure - 2]. The skin was fragile, the soles were normal, and the nails showed longitudinal ridging. A raised nodular lesion measuring around 1 x 1.5 cm was present on the left middle finger that was indurated and nontender. There was no ulceration or bleeding from the lesion. Routine blood investigations were normal. Excision biopsy was done and histopathological examination revealed a reactive epithelial hyperplasia with no evidence of malignancy. Based on the history and clinical findings, we made a diagnosis of Huriez syndrome. The patient was given topical tazarotene and advised to report back if new keratotic lesions appeared. Huriez syndrome is a rare autosomal dominant keratoderma characterized by scleroatrophy of the palmar skin. The soles are not commonly involved. [1] In addition to its occurrence in French patients, it has also been reported in Tunisia, Germany and Italy. [3] In our case, there was no history of consanguinity and none of the patient′s relatives were affected. Affected individuals carry a > 100-fold higher risk for the development of aggressive SCC of the skin. [4] The age at the onset of skin cancer is much lower than in the general population, and tumors arise in the areas of affected skin. Our patient had scleroatrophy from birth. He had recurrent fissuring with hyperhidrosis from early infancy and developed SCC at a very early age. Sclerosis, atrophy, and scarring [5] are well-recognized risk factors for the development of SCC of the skin. Clinically, the development of SCC in Huriez syndrome bears a striking similarity to Marjolin′s ulcer, which refers to malignancies arising in chronic ulcers of the skin, scar tissue, and burn scars. In our patient, the palmar skin was fragile and it has been observed that skin fragility found in Huriez syndrome leads to scarring, and the scleroatrophic changes may represent a process similar to scarring, thus predisposing the patient to skin cancer. In addition, the exposure to exogenous mutagens such as arsenic, has been recognized as a risk factor for the development of SCC. Watanabe et al, [3] found positive staining of p53 in atypical keratinocytes in their patient and suggested that p53 mutations may be responsible for development of actinic keratoses and squamous cell carcinoma in cases of Huriez syndrome. However, most PPKs are not associated with an increased risk of skin cancer. Nail changes such as hypoplasia, longitudinal ridging, and distal splitting are observed in Huriez syndrome. [3] Our patient had longitudinal ridging of the fingernails. It is noteworthy that loss of heterozygosity of 4q has been reported in Huriez syndrome. [1] However, we did not perform any genetic studies in our patient. Furthermore, immunohistochemically demonstrated depletion of Langerhans cells in the affected skin is also attributed to be a cause for epidermal carcinogenesis. [3] Identification and characterization of the gene causing Huriez syndrome may provide important insights into the pathogenesis of skin cancer. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08183f2.jpg] [dv08183f1.jpg] |
| |||||||||

{kind=link}
{kind=link}