
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 4, 2008, pp. 415-419
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 415-419
Focus
Techniques of immunofluorescence and their significance
Mohan KH, Pai Sathish, Rao Raghavendra, Sripathi H, Prabhu Smitha
Department of Skin and STD, Kasturba Medical College, Manipal
Correspondence Address:Department of Skin and STD, Kasturba Medical College, Manipal- 576 104, Udupi Dist, Karnataka
mohankudur@rediffmail.com
Code Number: dv08185
Immunofluorescence is a histochemical laboratory staining technique used for demonstrating the presence of antibodies bound to antigens in tissues or circulating body fluids. These techniques are essential to supplement clinical findings and histopathology in the diagnosis of immunobullous disorders. They permit early diagnosis, treatment, and subsequent monitoring of disease activity in patients with these potentially life-threatening disorders.
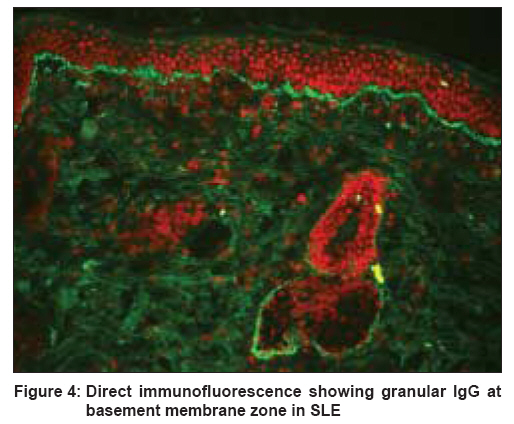
In 1941, Coons et al, developed the technique of immunofluorescence. Subsequently, granular deposits of IgG and C3 were first described along the dermo-epidermal junction in lesions of lupus erythematosus in 1963. In 1964, Beutner and Jordon used the indirect immunofluorescence (IIF) technique to demonstrate antibodies in the sera of pemphigus patients.
Immunofluorescence Techniques
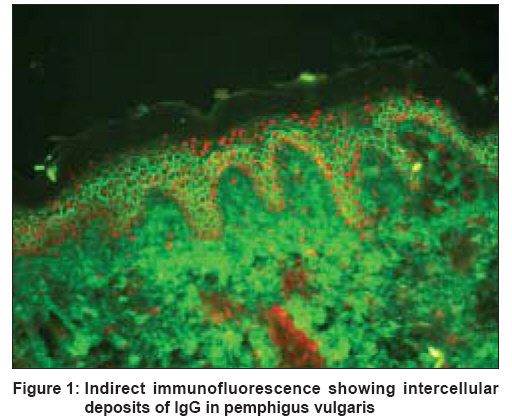
In clinical immunodermatology, there are three basic types of immunofluorescence techniques: direct immunofluorescence (DIF), indirect immunofluorescence (IIF) [Figure - 1], and complement binding indirect immunofluorescence. [1] All these methods entail the use of fluorescein-linked antibodies to immunoglobulins, complement components, or other proteins.
Fluorescent techniques involve the emission of light of one color/wavelength and a low energy level from a substance being irradiated with light of a different wavelength. Fluorescein isothiocyanate (FITC) and tetramethyl rhodamine isothiocyanate (TRITC) are two routinely used fluorochromes. The antibody is linked with fluorescein isothiocyanate (FITC) via a thiocarbamide linkage without destroying its capacity to react with the corresponding antigen.
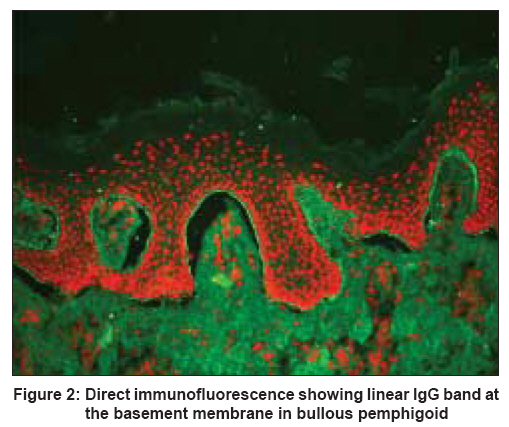
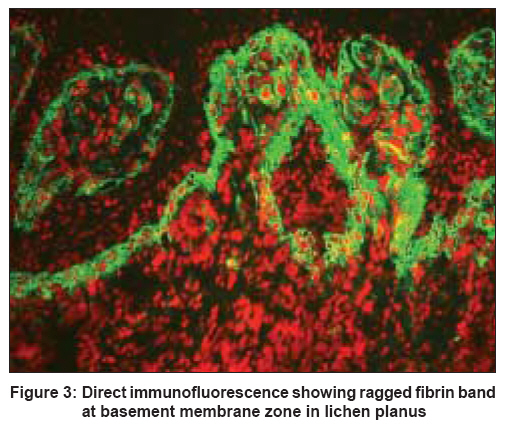
Direct Immunofluorescense This is a one-step histological staining procedure for identifying in vivo antibodies that are bound to tissue antigens. [1],[2] [Figure - 1],[Figure - 2],[Figure - 3] The procedure entails the following steps:
- Skin or mucosal biopsy specimens are usually obtained by 3-5 mm punch or surgical biopsy.
- Biopsy specimens are snap frozen . If there is a delay between biopsy and snap freezing, the specimen should be kept in cold saline.
- Frozen 4-6μ sections are cut on a cryostat and placed on a glass slide before being air-dried for 15 minutes.
- After rinsing in phosphate buffered saline (PBS), pH 7.2, slides are overlaid in a moist chamber with FITC conjugates with the following specificities: antiIgG, antiIgM, antiIgA, antiC3, and antifibrin. Each reagent is tested on a separate slide.
- After rinsing in PBS, slides are mounted in buffered glycerin and examined under a fluorescence microscope.
Indirect Immunofluorescence IIF is a two-step serological technique for detection of circulating antibodies in body fluids. [1],[2] The procedure involves the following steps:
- Substrate sections are allowed to react with serially diluted (1:10, 1:80 etc) patient′s serum in a moist chamber for 30 min. Control sera of known positive and negative antibody reactivity are tested simultaneously.
- Following a rinse in PBS to remove unbound serum proteins, sections are treated with a FITC-conjugated antiIgG or other antibody conjugates of defined specificity.
- Following a rinse for at least 10 min in PBS to remove the unbound conjugate, slides are mounted and examined under a fluorescence microscope.
Complement Indirect Immunofluorescence[1]
Antigens and antibodies bind to one another to generate many molecules of complement 3 (C3). This amplification principle is used in complement IIF, which is more sensitive than IIF. It is a three-step technique:
- A normal tissue substrate is overlaid with plasma, serum/other tissue fluid which has been heated to 56°C for 30 min to destroy the complement-fixing activity of antigen-antibody complexes. Specimens are then washed.
- Tissue sections are incubated with a source of complement such as fresh human serum. Complement-fixing IgG/IgM antibodies that have bound to the antigen in the first step can now activate complement, giving rise to numerous C3 molecules that are bound at the antigen-antibody binding site in the tissue. Specimens are then washed again.
- Sections are incubated with fluorescein-labeled antihuman C3 antibodies. These bind to C3 generated in the second step. After washing, the C3-antibody conjugates can be examined under a fluorescence microscope.
In some situations, so few IgG or IgM antibodies bind to tissue antigens that they cannot be detected by IIF. However, as these antibody-antigen complexes generate many C3 molecules, complement IIF is helpful to detect antigen(s) in these conditions.
Variants of Indirect Immunofluorescence
Salt split technique
This technique is used to distinguish between subepidermal blistering conditions with similar direct immunofluorescence findings. In this procedure, normal human skin is incubated in 1 M NaCl (sodium chloride) for 48-72 h to split it at the level of the lamina lucida. Bullous pemphigoid antibodies bind to the roof and floor of the blister while epidermolysis bullosa aquisita antibodies bind solely to the dermal (floor) side of the split skin.
Antigenic mapping method
This method is used as an adjunct to electron microscopy to differentiate between the major forms of epidermolysis bullosa . A blister is induced by rubbing the skin with a pencil eraser for one minute and a biopsy is taken from that area after ten minutes. The biopsy material is snap frozen and slides are prepared.
Indirect immunofluorescence is performed with polyclonal/monoclonal primary antibodies directed against different antigenic components of the dermal-epidermal junction, including the bullous pemphigoid antigen, laminin, and type 4 collagen. The cleavage plane is determined by noting which antigens are detected on the roof and the floor of the mechanically induced blisters. All three antigens are seen on the floor (intraepidermal split) in superficial blisters, bullous pemphigoid and laminin antigens are seen on the roof and type 4 collagen on the floor (intralamina lucida split) in junctional blisters, and all three antigens are detected on the roof (sublamina densa split) in dystrophic blisters.
Double staining method
In this method, FITC is used in conjunction with TRITC to demonstrate the co-distribution of two antigenic substances in tissues. Double staining can be used as a direct/indirect method. The indirect method has very high sensitivity.
Significance of indirect immunofluorescence
During active disease, 80-90% of pemphigus vulgaris patients show IgG antibody against the intercellular cement substance of stratified cornified epithelium. Circulating antibodies may not be detectable in early cases when there are only a few lesions, and during remission.
In pemphigus, titers of circulating intercellular antibodies can be correlated with disease activity-a two-fold rise in titer may indicate an impending relapse. [3],[4] Of the four classes of IgG, IgG1 is the best indicator of disease. False positive pemphigus-like antibodies have been reported in thermal burns, toxic epidermal necrlysis, SLE, lichen planus , healthy people, relatives of patients with pemphigus, D-penicillamine therapy, myasthenia gravis, trichophyton rubrum fungal infection, and lepromatous leprosy.
IIF can be used to demonstrate lichen planus specific antigen (LPSA), which is expressed in the stratum granulosum and stratum spinosum. LPSA is specific for lichen planus and found in 80% of patients with and without oral lesions.
On the other hand, direct immunofluorescence is believed to be virtually free of false positive results.
False negative results are seen with organ-specific antibody, prozone interference by the other antibodies, or due to error in technique.
Collection and handling of specimens for immunofluorescent studies in skin disease
Two types of specimens can be examined by IF techniques, notably biopsy specimens of skin or mucus membranes and serum samples. [5]
Biopsy specimens
Perilesional skin is used for immunofluorescence for DIF patients. Monkey or guinea pig esophagus, rat bladder epithelium for paraneoplastic pemphigus, or blister fluid can be used for IIF. Quick freezing is the most widely used method for handling biopsy specimens for IF studies. This can be performed by immersing the biopsy specimen either in liquid nitrogen or cold solid carbon dioxide or in a hexane bath. The quick frozen biopsy is then mounted in tissue-embedding compound and sectioned in a cryostat. Tissue substrates for IIF techniques are processed similarly. At present, immunofluorescence can be performed with biopsy specimens handled for several days at ambient temperature in a preservative liquid medium, as described by Michel et al . Michel′s medium is now commercially available.
Serum samples
Blood (8-10 mL) should be collected without anticoagulant. Serum is separated from the clotted blood and if not immediately tested, it should be aliquoted and stored at -20°C.
Other specimens for DIF
Outer root sheath of anagen hair from pemphigus vulgaris patients can be used for DIF. The outer root sheath is structurally analogous to epidermal keratinocytes in which antibodies can be detected.
Immunofluorescence findings in skin diseases
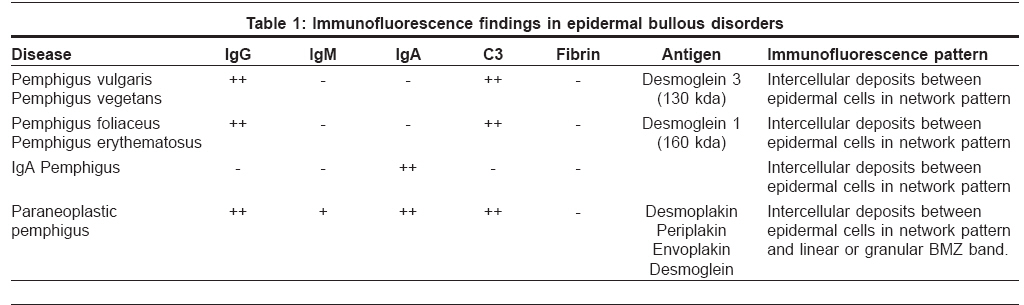
Immnufluorescence findings in the pemphigus group of diseases are tabulated in [Table - 1].
Immunoluorescence-negative bullous disorders
Immunofluorescence is negative in subcorneal pustular dermatosis, transient acantholytic dermatosis, familial benign chronic pemphigus, and epidermolysis bullosa. [6],[7]
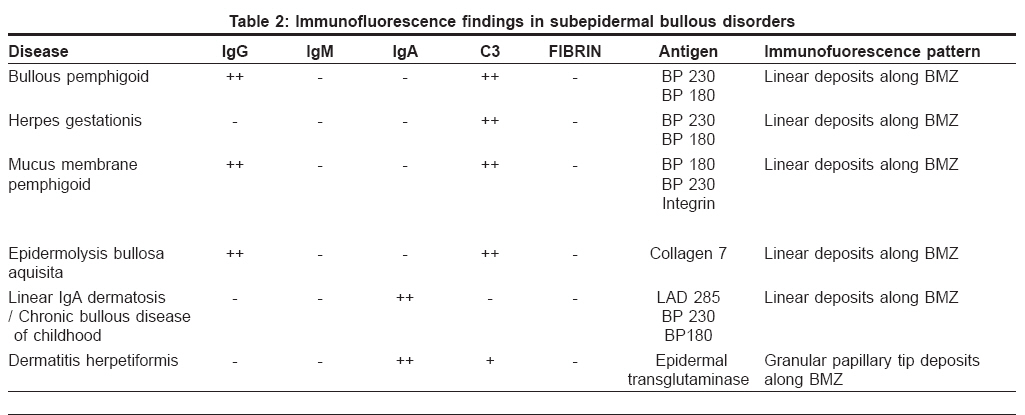
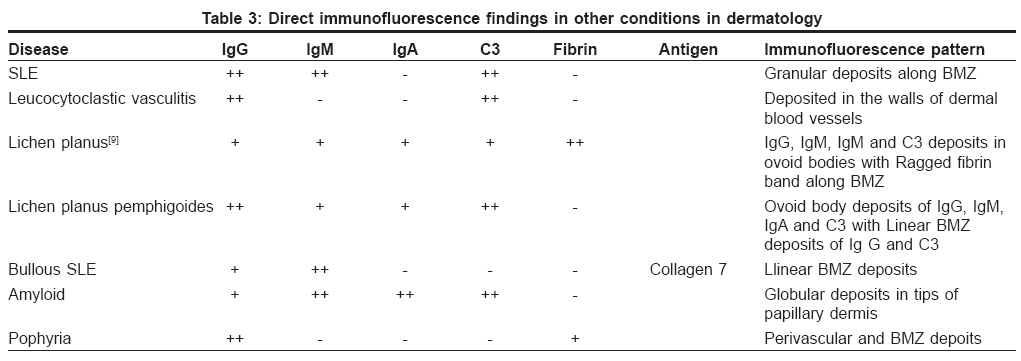
Immunfluorescence findings in subepidermal [Table - 2] and other skin diseases are enumerated [Table - 3]. [8],[9]
In conclusion, immunofluorescence methods provide a useful adjunct to light microscopy for reaching diagnosis of immunological skin diseases. However, they require technical skill to perform as well as experience and caution to interpret.[Figure - 4]
References
| 1. | Huligol SC, Bhogal BS, Black MM. Immunofluorescence of the immunobullous disorders: Part one: Methodology. Indian J Dermatol Venereol Leprol 1995;61:187-95. Back to cited text no. 1 |
| 2. | Vassileva S. Immunofluorescence in Dermatology. Int J Dermatol 1993;32:153-61. Back to cited text no. 2 [PUBMED] |
| 3. | Jablonska S, Chlorzelski T, Blaszyk M, Maciejewski W. Pathogenesis of pemphigus erythematosus. Arch Dermatol Res 1977;258:135-40. Back to cited text no. 3 |
| 4. | Chlorzelski TP, Butneur EH. Factors contributing to occasional failure in demonstration of pemphigus antibodies by immunofluorescence test. J Invest Dermatol 1969:53:188-91. Back to cited text no. 4 |
| 5. | Rao R, Shenoi SD. Indirect immunofluorescence to demonstrate lichen planus specific antigen (LPSA) in Lichen planus. Indian J Dermatol Venereol Leprol 2006;72:350-2. Back to cited text no. 5 |
| 6. | Feliciana C, Pour SM ,Toto P, Coscione G, Amerio P. Direct immunofluorescence diagnosis of pemphigus without biopsy. J Cutan Med Surg 1998;2:209-11. Back to cited text no. 6 |
| 7. | Brystryn JC, Sabolinski M. Effect of substrate on indirect immunofluorescence tests for intercellular and basement membrane zone antibodies. J Am Acad Dermatol 1986;15:973-7. Back to cited text no. 7 |
| 8. | Ratnam KV, Pang BK. Pemphigus in Remission: Value of negative Direct Immunofluorescence in management. J Am Acad Dermatol 1994;30:547-50. Back to cited text no. 8 [PUBMED] |
| 9. | Bhogal B, Wojnarowska F, Black MM, Xu W, Levene GM. The distribution of immunoglobulins and the C3 component of complement in multiple biopsies from the uninvolved and perilesional skin in pemphigus. Clin Exp Dermatol 1986;11:49-53. Back to cited text no. 9 [PUBMED] |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08185f4.jpg]
[dv08185t2.jpg]
[dv08185f2.jpg]
[dv08185t1.jpg]
[dv08185t3.jpg]
[dv08185f1.jpg]
[dv08185f3.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}