 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 420-423 Resident's Page Scars in dermatology: Clinical significance Anitha B, Ragunatha S, Inamadar ArunC Department of Dermatology, Venereology and Leprosy, BLDEA's SBMP Medical College, Hospital and Research Centre, Bijapur, Karnataka Code Number: dv08186 A scar is a scar is a scar and only a scar if you don′t ask why" A scar is a fibrous tissue replacement that develops as a consequence of healing at the site of a prior ulcer or wound. Cutaneous scarring is a macroscopic disturbance of the normal structure and function of the skin architecture manifesting itself as an elevated or depressed area, with an alteration of skin texture, color, vascularity, nerve supply and biomechanical properties. [1] Histologically, dermal scars are characterized by thickened epidermis with a flattened dermo-epidermal junction and an abnormal organization of the dermal matrix into parallel bundles of scar tissue collagen, as opposed to the normal basket weave pattern of dermal collagen. Scar collagen fibers have high proportions of type III collagen and fibronectin compared to the surrounding normal skin and are usually smaller and more densely packed. Elastic fibers are fragmented and abnormally organized in scars as compared to the normal dermis. Epidermal appendages such as hair follicles and sebaceous glands are usually absent in a scar. [1] The pathogenesis of raised skin scars is unclear. Fibroblasts from hypertropic scars and keloids demonstrate excessive proliferative and low apoptosis properties. Fibrogenic isoforms of transforming growth factor β (TGF β 1, 2, 3 ) appear to play a central role in the pathogenesis process. TGF β 1 stimulates fibroblasts leading to proliferation and synthesis of procollagen RNA and hence, collagen formation. By upregulating the production of tissue inhibitor metalloproteinase and plasminogen activator inhibitor, TGF β 1 protects the collagen from degradation. [2] Classification of Scars[3]
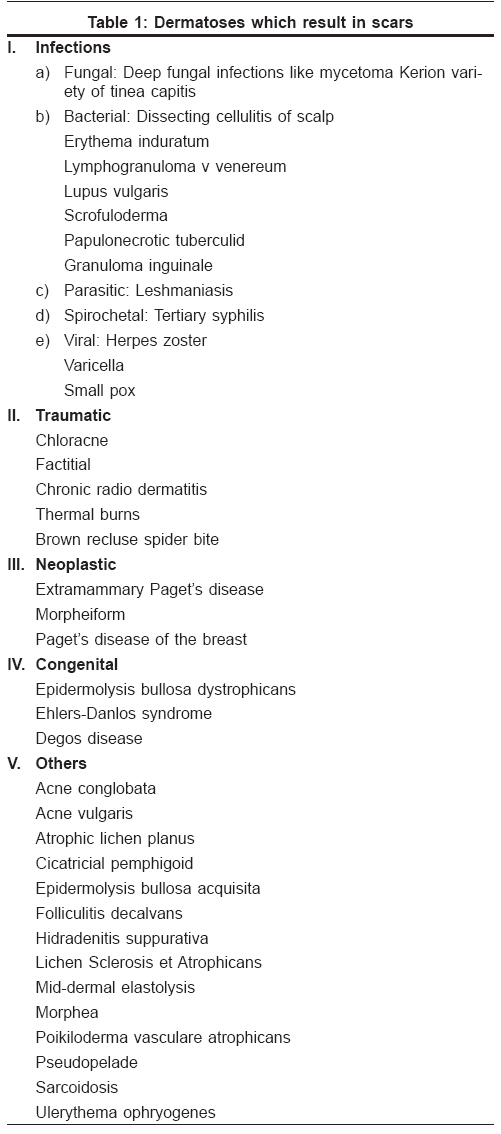
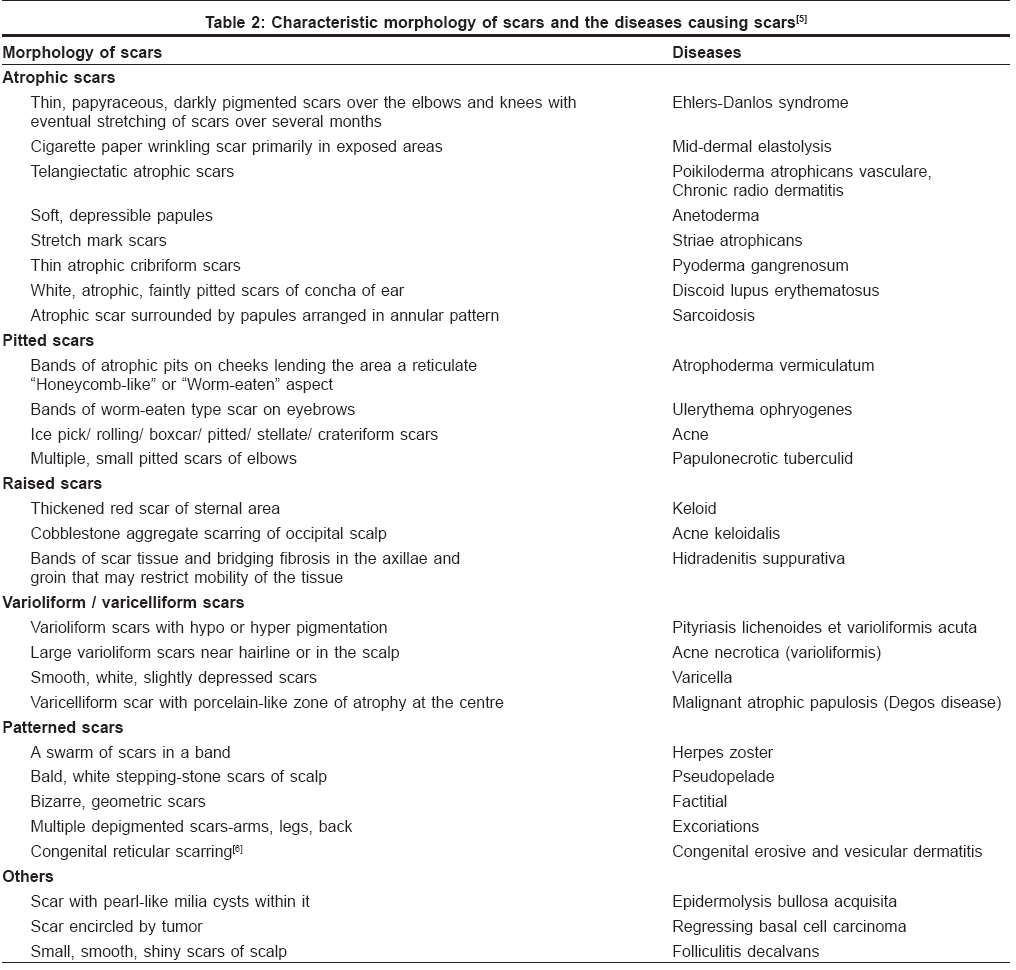
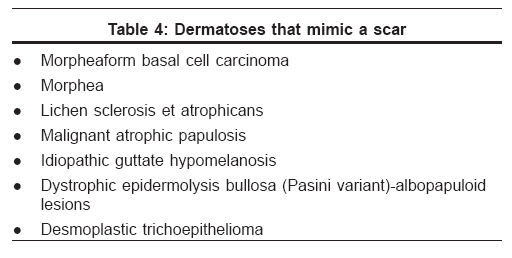
Dermatological Conditions Which Result in Scars Many dermatological disorders can lead to cutaneous scarring. [Table - 1] enumerates a few of these conditions: [4] Scars do not just occur as a consequence of the healing process, but also have other clinical significance. They may serve as a clue for diagnosis by their typical morphology or may give rise to various dermatoses while some dermatoses may mimic scars. These aspects of scars are discussed below. Morphology of Scars as a Clue for Diagnosis[Figure - 1],[Figure - 2],[Figure - 3] Dermatological Conditions Occurring in Scars Certain dermatological conditions arise from a scar and have a tendency to recur within the scar tissue. These disorders may occur in scars as a result of Koebner′s phenomenon, inoculation of infectious agents, metastases or long-standing changes in the scars [Table - 3]. In pseudoxanthoma elasticum, the disease process can be demonstrated in scars before the appearance of skin lesions. In such cases, a biopsy of the scar has been used for diagnosis of the disease. [7]Dermatoses Mimicking Scars Some dermatoses may clinically mimic a scar requiring careful examination and histopathological studies to confirm the diagnosis. The absence of history of prior injury should raise suspicion of these disorders [Table - 4].Spontaneous Scarring and Pseudoscars Scars can occur without any history of previous trauma. These tend to occur in predisposed individuals. However, there may be prior trivial trauma, hemorrhage [10] or dermatitis unnoticed by the patient. [11] Atrophia maculosa varioliformis cutis: In this condition, spontaneous atrophic linear, rectangular or varioliform scars with sharp margins develop over the cheeks of children and young adults. [11] Stellate and discoid pseudoscars: Stellate pseudoscars are white, irregular or star-shaped atrophic scars occurring over the sun-exposed areas of the forearms. It is commonly seen in elderly individuals aged 70-90 years. Brown pseudoscars are known to occur over the shins of patients with diabetic dermopathy. [10] In most of the cases, except for cosmetic unacceptability, a scar is not a cause for much concern. However, a simple scar can be a site for the development of various dermatoses or it can undergo neoplastic changes over time. Hence, any long-standing scar with or without morphological changes, should be examined carefully and should be biopsied if necessary. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08186f2.jpg] [dv08186t1.jpg] [dv08186t2.jpg] [dv08186f1.jpg] [dv08186t4.jpg] [dv08186f3.jpg] [dv08186t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}