 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
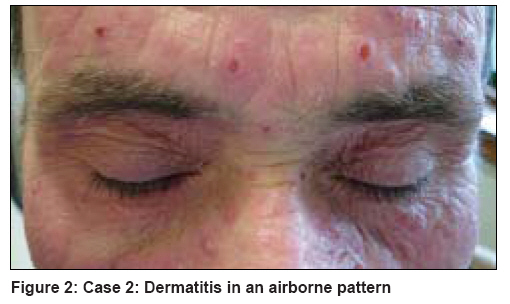
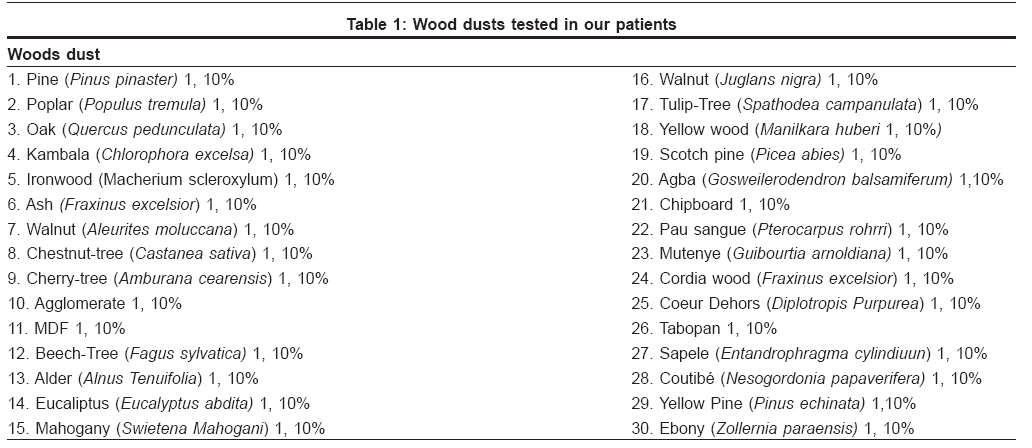
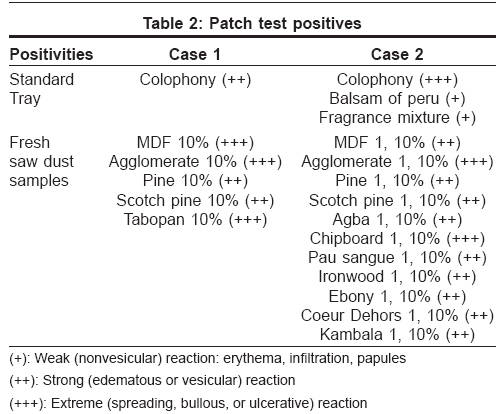
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 431 Net letter Contact dermatitis in Wood workers Lobo I, Ferreira M, Silva E, Machado S, Selores M Department of Dermatology, Hospital Geral de Santo António, EPE, Porto Code Number: dv08193 Sir, Wood and wood dust can cause a wide range of cutaneous reactions, including folliculitis, contact urticaria, and both irritant and allergic contact dermatitis. The majority of wood-induced contact dermatitis occurs in woodworkers [1] and most involved sawdust woods are "exotic" species from tropical regions. [2] Solid wood products such as musical instruments are rarely sensitizing. [3] As exposure in woodworkers occurs with fine dust created during wood processing, the initial clinical picture is typically that of airborne contact dermatitis. Case 1 The physical examination [Figure - 1] revealed erythema, small vesicles, and scaling on the face (involvement of the eyelids, postauricular and infranasal folds), jaw area, neck and the V of the chest, hands and forearms. These episodes were so severe that they needed repeated visits to emergency service and the need of systemic corticosteroids. Case 2 Patch tests in both patients were performed with the Portuguese Contact Dermatitis Standard Tray, and fresh sawdust samples from 30 wood samples in 1 and 10% petrolatum [Table - 1]. The patches were applied with Finn chambers to the skin on the back, removed after 48 hours and read by 72 hours. After 72 hours, the first patient revealed positive reactions to colophony and five saw dusts in 10% petrolatum (MDF, agglomerate, pine, Scotch pine and Tabopan) [Table - 2]. The second patient demonstrated positivity to colophony, balsam of peru, fragrance mix and 11 saw dusts incorporated in 1 and 10% petrolatum (MDF, agglomerate, pine, Scotch pine, Agba, chipboard, Pau sangue, ironwood, ebony, Coeur dehors and kambala, [Table - 2]. Considering that many woods have strong irritant properties and that the first patient only revealed positive results to sawdust in 10% petrolatum, patch tests with the same saw dusts were carried out in ten controls. All these controls were negative, negating the hypothesis of irritant contact dermatitis. However, this conclusion was limited by the small number of controls. As photo-exposed areas were involved in both patients, we carried out photopatch tests. Negativity in these tests permitted us to exclude photo-allergic contact dermatitis. Woods and wood handling can cause various skin and mucosal adverse symptoms. Almost any wood dust has the potential to be an irritant agent when it comes in contact with the skin. Nevertheless, occupational allergic contact dermatitis is rare. [4] The most recognizable allergic woods include cedar, pine, poplar, oak, rosewood, teak and ebony. [5] Quinones, stibenes, phenols and terpenes are some of the compounds that have been identified as contact allergens in woods. [5] When wood contact dermatitis is suspected on a clinical basis, patch testing should be performed with fresh sawdust from the same wood species crafted by the patient. [4] Although 2,6 dimethoxy-1,4 benzoquinone is considered to be a wood allergy marker, we could not perform any test with it because the substance was not available. The cases described here clearly show that airborne contact dermatitis occurs with the involvement of other woods besides "exotic" types. In the second patient, we can infer that the reaction was allergic, but the negativity to saw dusts in 1% petrolatum in the first patient does not allow us to exclude an irritant reaction. The positive patch test reaction to wood sawdust demonstrates clinical relevance because the patients work with these woods on a daily basis and the dermatitis resolves on its own whenever they avoid wood contact. It is interesting to note that the clinical manifestations appear for a long time after woodworking activity, apparently with no modification on the type of woods crafted. This may be justified by the multiplicity of some woods′ common names reported by our patients, which made wood identification somewhat difficult. Ideally, woods should be identified by their genus and species names. Colophony is the natural solid residue that remains after distilling the volatile oil (turpentine) of the pine oleoresin. The positivity in both patients seems to be related with pine dust positivity. Wood agglomerate, MDF, and Tabopan are produced by agglutinating wood-waste fibrous elements with the gum of formaldehyde. Taking into account that neither of our patients had positive reactions to formaldehyde, the positivity to these wood agglomerates seems to be in agreement with pine dust positivity. In spite of these facts, we cannot exclude the involvement of other unknown wood constituent elements. Prevention of allergic contact dermatitis to wood dust in sensitized workers is usually difficult. Both our patients needed to leave the woodworking activity to get long-term relief from the wood dust-associated contact dermatitis. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08193f1.jpg] [dv08193t2.jpg] [dv08193t1.jpg] [dv08193f2.jpg] |
| |||||||||

![Figure - 1]](/showimage?dv/photo/dv08193f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}