 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
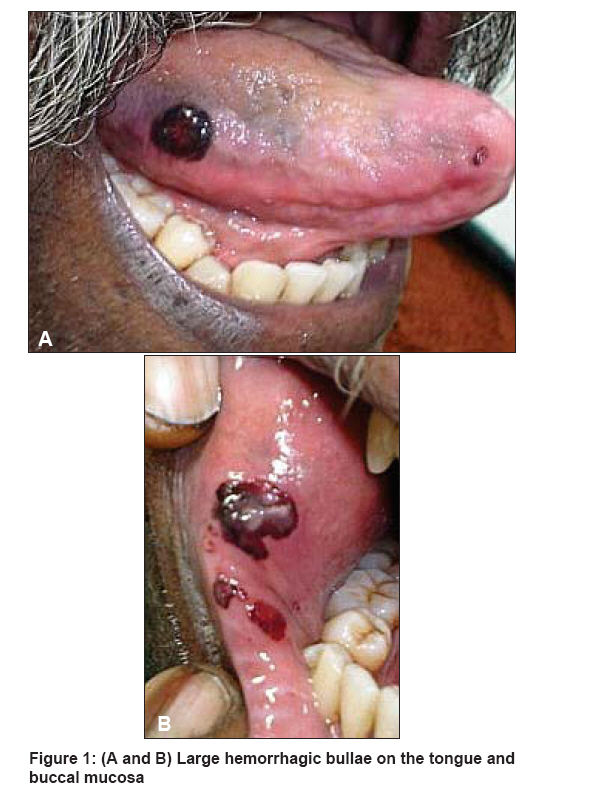
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 4, July-August, 2008, pp. 431 Net Quiz Hemorrhagic blisters in the mouth Narang Tarun, Kanwar AmrinderJ Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh Code Number: dv08194 A 44 year-old male presented with hemorrhagic blisters in the oral mucosa. He developed these lesions two days before presentation, after eating hot and spicy food. The lesions were painful and increased in size over the next 24 hours. He did not have any history of bleeding diathesis or any blistering disorder. The skin and mucosal examination revealed blood-filled blisters that were 2 mm to just over 1 cm in diameter on the buccal mucosa and tongue [Figure 1a and b]. Hematological and coagulation tests were normal. The patient was reassured about his condition and asked to follow up after two weeks. All the lesions had resolved without any sequelae after two weeks. What is your Diagnosis ? Diagnosis: Angina bullosa hemorrhagica (ABH)Discussion In 1967, Badham coined a new term, "angina bullosa hemorrhagica" (ABH) to describe oral blood-filled vesicles or bullae that could not be attributed to a blood dyscrasia, vesiculo-bullous disorder, systemic disease or other known causes. [1] Other names used to describe this condition are traumatic oral hemophlyctenosis and recurrent oral hemophlyctenosis. Kirtschig and Happle pointed out that the term ABH is misleading because most bullae arise in the oral cavity and are not consistent with lesions usually called "angina." They proposed a more appropriate name for the disease: stomatopompholyx hemorrhagica. [2] ABH is characterized by an acute and often painful onset of blood-filled blisters, mainly located at the junction of the hard and soft palate. Other nonkeratinized mucosal sites such as the buccal mucosa, the lateral and ventral borders of the tongue and the cheek mucosa may be involved, whereas the masticatory mucosa seems not to be affected. [3] The intact bulla is dark red to purple, has an ecchymotic halo and can be painful, but the pain disappears after rupture. The blister spontaneously ruptures after a short time and leaves a bleeding, ragged, often painless ulcer that heals spontaneously within one or two weeks without scarring. Peak incidence is in middle-aged and elderly patients. The history of each blistering episode is characteristic and similar for each patient. The lesions frequently develop during or immediately after meals. Some patients report a burning sensation before the onset of the blisters. [4] The bullae have been divided into two clinical groups: (i) solitary and large; and (ii) generalized and small. They appear suddenly, are often painless, and rupture shortly afterwards, releasing fresh blood. They typically develop during meals and usually heal without scarring in 7-10 days. Possible etiological factors include trauma, long-term use of steroids, diabetes, and hereditary predilection. No underlying hematological or immunopathological disorders have been identified. The subepithelial cleavage is followed by bleeding from the superficial capillaries resulting in the formation of hemorrhagic bullae. [3],[5] Although ABH can occur in the absence of concomitant drug intake, High and Main demonstrated a strong association between long-term inhalation of steroids and ABH, the latter becoming more common after 5-year use of steroid-based inhalers. [6] The diagnosis of ABH is largely clinical and includes the elimination of other disease processes through histological investigation. There are very few descriptions of the histopathology of ABH. It seems that extravasated blood from superficial vessels raises the overlying epithelium; in fact, a subepithelial separation from the lamina propria can be seen. A mild inflammatory reaction and parakeratosis can be present in the surrounding tissue. Direct immunofluorescence staining for IgA, IgG, IgM and fibrin is negative and can demonstrate equivocal staining along the basement membrane zone for C3. Biopsy and immunofluorescence studies may be useful to exclude other blistering diseases. [6] Lesions of ABH can be easily confused with those occurring in many dermatological and systemic disorders. Patients with bleeding disorders (thrombocytopenia and von Willebrand′s disease) and leukemia can present with intraoral blood-filled lesions. In Rendu-Osler-Weber disease, the angiomatoid lesions mimic bullae, but they are not episodic and other clinical and genetic features exist. History, clinical examination, coagulation and hemostatic function tests will distinguish these conditions from ABH. Several subepithelial bullous diseases including benign mucous membrane pemphigoid (BMMP or cicatricial mucous membrane pemphigoid), bullous pemphigoid (BP), dermatitis herpetiformis (DH), linear IgA disease (LAD), and bullous lichen planus (BLP) can be confused with ABH. The management of a patient presenting with oral blood-filled bullae should start with a detailed medical history and a careful examination to differentiate ABH from other more serious diseases. The lesion should be biopsied for histological investigations and direct immunofluorescence in order to exclude more serious diseases. A complete blood count and a baseline coagulation tests should always be performed to exclude hematologic disorders. No treatment is required and the patient should be reassured of the benign nature of the blisters. Large palatal or pharyngeal blisters causing a choking sensation should be broken if still intact. Management of these lesions should include the use of antiinflammatory or antibacterial rinses (0.25% chlorhexidine gluconate) to relieve pain and to limit secondary infections of the ulcers. Long-term follow-up is recommended to positively exclude other conditions which may present with oral blood-containing bullae. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08194f1.jpg] |
| |||||||||

{kind=link}