 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
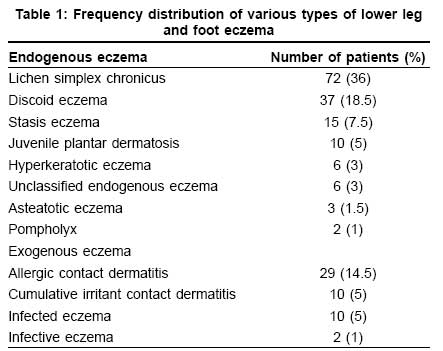
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 458-461 Original Article Patterns of lower leg and foot eczema in south India Chougule Abhijit, Thappa DevinderMohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: dv08199 Abstract Background: The pattern of eczema is altered by geography, habits of people and environmental factors and regional variation in skin structure and function.Aims: Our study was done to estimate frequency and patterns of lower leg and foot eczemas. Methods: A total of 200 patients with various types of lower leg and foot eczemas were recruited over a period of 2 years. Demographic and clinical characteristics were noted. Suspected cases of allergic contact dermatitis were patch tested. Results: The frequency of these eczemas was 2.5 per 1000 out patients. Mean age of patients was 40.49 years. Female to male ratio was 1.6:1. Sixty (30%) patients were farmers, sixty (30%) were housewives, forty (20%) were students, nineteen (9.5%) were daily laborers, nine had sedentary jobs and three were teachers. Most eczemas were bilateral (72%). Mean duration of eczema was 36.6 months. Most common type of eczema was lichen simplex chronicus (36%) followed by discoid eczema (18.5%), allergic contact dermatitis (14.5%) and stasis eczema (7.5%). Other eczemas noted were juvenile plantar dermatosis, cumulative irritant contact dermatitis, infected eczema, hyperkeratotic eczema, asteatotic eczema, pompholyx, infective eczema and unclassified endogenous eczema. Common sites of involvement were dorsa of feet (49.5%), followed by lateral aspect of lower leg (31%), medial aspect of lower leg (17.5%) and ankle (12%). Conclusion : Our study highlights lichen simplex chronicus as the most common eczema affecting the lower legs and feet. Keywords: Discoid eczemas, Eczemas, Lower leg, Lichen simplex chronicus Introduction Some forms of eczema are altered by regional variation in structure and function of the skin, and these may modify its appearance in regions such as hands and lower legs. [1] Legs and feet are affected by various eczemas. Classically stasis dermatitis affects lower legs. Other eczemas more likely to occur are nummular eczema, juvenile plantar dermatosis, pompholyx, lichen simplex chronicus and allergic contact dermatitis. They are usually chronic, recurrent and difficult to control. They may make patients unable to perform daily activities because of pain caused by fissures or because of secondary infections. They may prevent the wearing of shoes, especially when shoes are the cause of the dermatosis. There are many studies which give data regarding incidence and patterns of eczemas in general. Good data is available regarding the patterns of hand dermatitis but there is hardly any study on the patterns of lower leg and feet eczemas. Hence, we undertook this study to determine frequency and patterns of lower leg and foot eczemas. Methods It was a descriptive type of study conducted from August 2005 to June 2007 in the dermatology department at our institute. All consecutive patients of lower leg and foot eczema attending the dermatology out patient department (OPD) from August 2005 to June 2007 were included in the study after taking their consent. All patients who presented with predominant localized lower leg and foot eczema irrespective of their age and sex were included in our study. Those patients with air borne contact dermatitis or other type of widespread dermatitis and also involving the lower legs were excluded. Parameters studied were age, sex, duration, occupation, symptoms, contact history, site of involvement, and morphology. Ethical committee of the institute cleared the project. Diagnosis of eczemas involving lower leg and foot was made utilizing standard definitions accepted in the literature. [1],[2],[3],[4],[5],[6] After analyzing the history and clinical examination findings, type of dermatosis the patient was suffering from could be ascertained. Patients were prescribed appropriate medications and advised to visit after the lesions subsided. The data was tabulated and analyzed. Results Two hundred patients with eczema of lower leg and foot were included in this study. A total of 80,221 patients attended the Dermatology OPD during the study period. The frequency of lower leg and foot eczema in our study was 2.5 per 1000 patients attending the Dermatology OPD. Mean age of 200 patients in this study was 40.49 years with a standard deviation of 18.6 (range 1 year to 80 years), 122 (61%) were females and 78 (39%) were males, with female to male ratio of 1.6:1. The most common age group affected was 31-45 years (59 cases, 29.5%) followed by 46-60 years age group (55 cases, 27.5%), 16-30 years (39 cases, 19.5%), less than or equal to 15 years (24 cases, 12%), 61-75 years (21 cases, 10.5%) and more than 75 years age group (2 cases). Majority of the females (69 cases, 56.6%) were in 16-30 and 31-45 year age groups; whereas majority of the males (48 cases, 61.5%) were in 31-45 and 46-60 years age group. Majority of the study population (60 cases, 30%) were farmers, followed by housewives (60 cases, 30%), students (40 cases, 20%), daily wage laborers (19 cases, 9.5%), office workers (9 cases), and teachers (3 cases). Mean duration of eczema was 36.6 months and the range was 1 week to 20 years. Eleven cases had history suggestive of atopy. Eczemas were bilateral in 145 (72%) cases the rest (57, 28%) being unilateral. Two cases had stasis eczema and asteatotic eczema on both legs along with unilateral LSC. Sites of involvement in decreasing order of frequency were as follows: dorsum of foot (99 cases, 49.5%), lateral aspect of lower leg (62 cases, 31%), medial aspect of lower leg (35 cases, 17.5%), ankle (24 cases, 12%), dorsum of toes (19 cases, 9.5%), instep of sole (18 cases, 9%), fore sole (16 cases, 8%), toe web spaces (13 cases, 6.5%), plantar aspect of toes (10 cases, 5%), posterior aspect of feet (8 cases, 4%), margins of feet (4 cases, 2%), hind sole (3 cases, 1.5%) and posterior aspect of leg (1 case, 0.5%). A total of 12 types of lower leg and foot eczema were noted in this study [Table - 1]. Correlation with clinical parameters Gender and type of eczema: Gender had no bearing on the occurrence of lichen simplex chronicus and discoid eczema. However some eczemas such as cumulative irritant contact dermatitis and pompholyx were exclusively observed in female patients. Stasis eczema and asteatotic eczema were relatively infrequent in female patients. Occupation and type of eczema : Stasis eczema was found to be common in farmers (9 out of 15 cases) and cumulative irritant contact dermatitis in housewives (6 out of 10 cases). The most common types of eczema in students were juvenile plantar dermatosis (10 out of 40 cases) and allergic contact dermatitis (9 out of 40 cases). In daily wage workers lichen simplex chronicus, (7 out of 19 cases) was the most common eczema followed by discoid eczema (5 out of 19 cases). In office workers, the most common eczema found was lichen simplex chronicus (7 out of 19 cases). Duration and type of eczema: In most cases of allergic contact dermatitis (16 out of 29 cases), infected eczema (9 out of 10 cases) and pompholyx (2 out of 2 cases), the duration of eczema was 6 months or less. Most cases of lichen simplex chronicus (56 out of 72 cases), discoid eczema (29 out of 37 cases), stasis dermatitis (11 out of 15 cases), cumulative irritant contact dermatitis (8 out of 10 cases), juvenile planar dermatosis (8 out of 10 cases), hyperkeratotic eczema (4 out of 6 cases) and asteatotic eczema (2 out of 3 cases) had their disease for 6 months to 5 years. The unclassified endogenous eczemas were of more than 5 years duration. History of atopy and eczema: History of atopy was present in discoid eczema (5 out of 37 cases), allergic contact dermatitis (3 out of 29 cases), juvenile plantar dermatosis (2 out of 10 cases) and cumulative irritant contact dermatitis (1 out of 10 cases). Distribution and type of eczema: Although unilateral distribution was sometimes seen, the following types of eczemas were predominantly bilateral: lichen simplex chronicus, discoid eczema, allergic contact dermatitis, stasis eczema, and infected eczema. Unilateral distribution was not seen in the following types of eczema: juvenile plantar dermatosis, cumulative irritant contact dermatitis (CICD), hyperkeratotic eczema and asteatotic eczema. Site of involvement and type of eczema: Juvenile plantar dermatosis, hyperkeratotic eczema, pompholyx and asteatotic eczemas were diagnosed because of their distinctive morphology and sites of involvement. Dorsum of foot was involved in lichen simplex chronicus (32 cases, 16%), discoid eczema (26 cases, 13%), allergic contact dermatitis(23 cases, 11.5%) and stasis eczema (8 out of 15 cases). Lateral aspect of leg was involved in lichen simplex chronicus (29 cases, 14.5%), discoid eczema (20 cases, 10%). Medial aspect of leg was involved in 15 out of 15 cases of stasis eczema. Ankle was involved in LSC in 19 cases (9.5%). Instep of sole was involved in 9 out of 10 cases of CICD and 2 out of 2 cases of pompholyx. Toe web spaces were involved in 8 out of 10 cases of CICD. Out of 29 patients of allergic contact dermatitis, 21 patients consented for patch testing with the Indian standard series of allergens approved by Contact and Occupational Dermatoses Forum of India (CODFI). Eight patients showed positive (allergic) patch test reaction to at least one allergen. Five out of 13 patients who were suspected to have footwear allergic contact dermatitis got positive results. Among these five patients, thiuram mix gave three positive reactions; fragrance mix gave two positive; nickel, black rubber mix and epoxy resin each gave one positive reaction. Hence rubber chemicals (thiuram mix, black rubber mix and epoxy resin) were found to be the commonest allergens in our study. Discussion Hanifin et al . reported most frequent ages at onset for empirically defined eczema in a population based survey of eczema in the range of 18 to 29 years. [7] The age of patients in present study ranged from 1 year to 80 years with a mean of 40.5 years. Most patients belonged to 31-60 year age group. Lichen simplex chronicus (88.9%) was the predominant group of lower leg and foot eczema. Lichen simplex chronicus may be primary (arising on tissue with a normal appearance) or secondary (superimposed on other underlying disease). It occurs most commonly between the ages of 30-50 years. [1] All the cases of LSC in our study were presumed to be primary. Almost any area may be affected by LSC, but most common sites are those that are conveniently reached. It can be either unilateral or bilateral reflecting a preference for scratching with the dominant hand. [1],[8] Stasis eczema typically affects middle-aged or elderly, especially female, patients and rarely occurs before the fifth decade of life, except in patients with acquired venous insufficiency. In a study of incidence of various types of eczemas over 27 years in Ipswich, UK, gravitational eczema was recorded in 4% cases. [1] In our study, stasis eczema was observed in 15 cases (7.5%) out of a total 200 cases of lower leg and foot eczema, with a mean age of 55.6 years. This eczema was seen most commonly in farmers (9 cases), as they are involved in standing as well as mobile field work. Jones et al . [9] reported 102 cases of juvenile plantar dermatosis, mean age at onset of disease was 7.3 years and the mean duration of disease was 8.4 years. In our study, juvenile plantar dermatosis was observed in 10 cases (5%) and the findings were in concurrence with the literature. This eczema was observed only in students, may be because of consistent use of shoes and socks during school time. High incidence of atopy reported observed by Ashton et al . [10] was not a feature of our study. Cumulative irritant contact dermatitis (wear and tear dermatitis) develops as a consequence of multiple incidents of sub threshold damage to the skin and was a unique feature of our study. It was observed in 10 cases (5%), with a mean age of 28.3 years. This eczema was observed most commonly in housewives (6 cases), probably because many Indian housewives are involved with household work including washing clothes and utensils with detergents and water. All 10 cases had bilateral eczema, involving most commonly insteps of soles (9 cases) and toe web spaces (8 cases) followed by margins of feet, and dorsal aspect of toes. This is probably because many of them squat on the ground; and their feet are continuously exposed to detergents and water. Hyperkeratotic eczema occurs commonly in middle-aged to elderly men and is normally very refractory to treatment whereas asteatotic eczema commonly occurs on the shins of elderly patients. [11] Clinically, there are several forms of asteatotic eczema which are either localized or generalized and which have different implications. [12] Asteatotic eczema of legs was observed in three cases (1.5%) in our study. Infective eczema is an eczema that is caused by microorganisms or their products, and which clears when organisms are eradicated. It must be distinguished from infected eczema in which eczema resulting from some other cause is complicated by secondary bacterial or viral invasion of the broken skin. These two conditions may coexist and distinction can be difficult. [1] In the present study, infected eczema affecting lower legs and feet were observed in 10 cases (5%) while infective eczema was observed in two cases (1%) only. Allergic contact dermatitis of legs and feet is mainly associated with the use of footwear and topical medicaments for eczema. [5],[13] In the present study, allergic contact dermatitis was suspected in 29 cases (14.5%). Five out of 13 patients who were suspected to have footwear allergic contact dermatitis had positive patch test results. To conclude, most common type of eczema affecting lower legs and feet in our study was lichen simplex chronicus (72 cases, 36%) followed by discoid eczema (37 cases, 18.5%), allergic contact dermatitis (29 cases, 14.5%) and stasis eczema (15 cases, 7.5%). The most common site of involvement was dorsum of foot (99 cases, 49.5%), followed by lateral aspect of lower leg (62 cases, 31%), medial aspect of lower leg (35 cases, 17.5%) and ankle (24 cases, 12%). We observed a special type of eczema in Indian housewives which involves toe web spaces and instep of soles, suggesting cumulative irritant contact dermatitis. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08199t1.jpg] |
| |||||||||

{kind=link}