 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
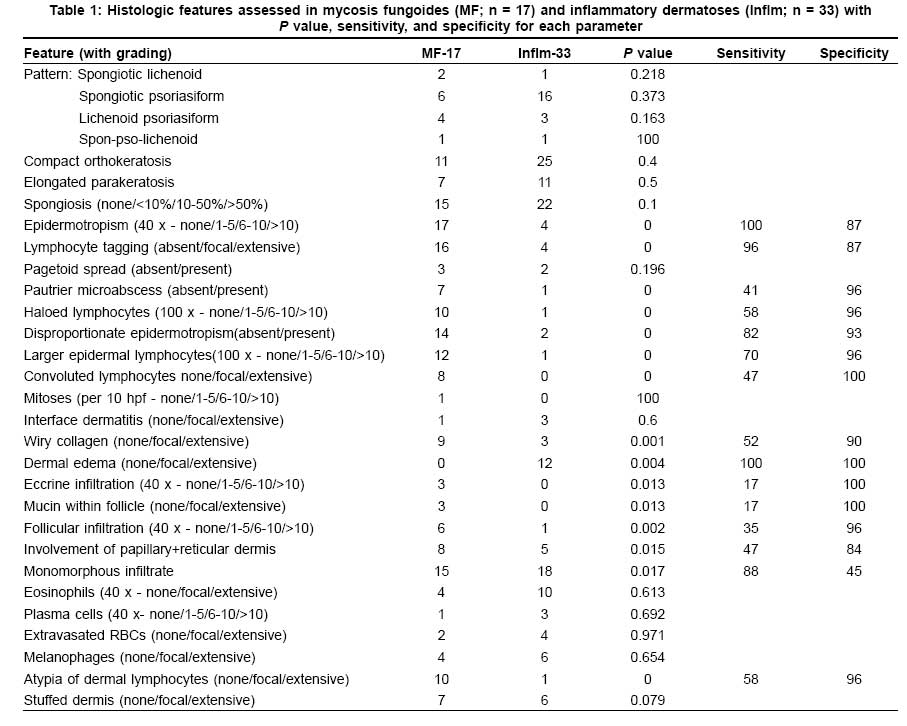
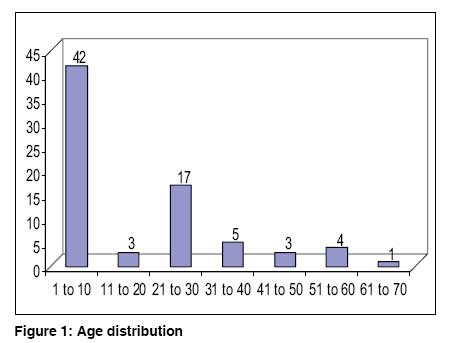
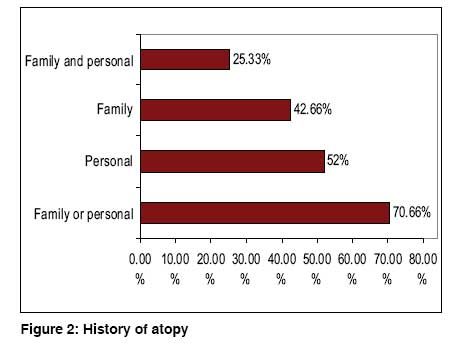
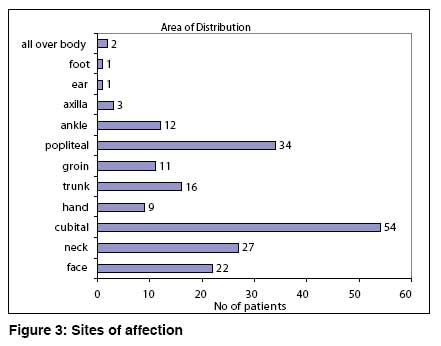
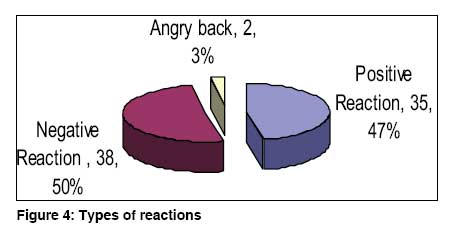
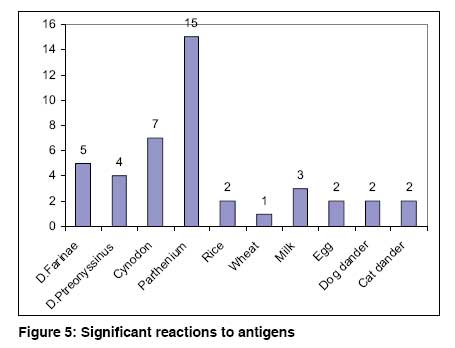
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 467-470 Brief Report Atopic patch testing Krupa Shankar DS, Chakravarthi M Manipal Hospital, Bangalore Code Number: dv08201 Abstract Background: Atopic dermatitis is a major problem among the urban population and it can be aggravated or triggered by various allergens. Atopic patch test can be used as a diagnostic tool in characterizing patients with allergen triggered atopic dermatitis.Aims: 1. Patch testing to reproduce an eczematous reaction by applying prick test allergens under occlussion on intact skin. 2. To find the allergen associated with atopic dermatitis. 3. To find the specific allergen which causes or exacerbates atopic dermatitis in a given subject. Methods: Seventy five subjects with atopic dermatitis were included in our study and patch tests using prick test allergens were applied to the back. Reading was done after 48 and 72hours Results: Out of the 75 subjects tested, 47% showed positive reactions, parthenium accounted for 42% of all positive reactions. Conclusions: Epicutaneous application of prick test antigen on intact skin can produce a reaction. Parthenium is commonest allergen in Bangalore. Counselling based on patch test reports may help to reduce morbidity and improve quality of life. Keywords: Atopic dermatitis, Atopic patch, Prick test allergen, Skin prick test Introduction Atopic dermatitis is a chronic inflammatory skin disorder characterized by intense itching and a relapsing course especially in infants and children with a personal or family history of atopic disorders. Several new aspects with regard to the pathogenetic background as well as strategies for prevention, diagnosis and treatment in atopic dermatitis have emerged. There are ongoing studies on genetic susceptibility loci, as well as environmental and nutritional factors associated with an increase or a decrease of atopic dermatitis lesions. The atopic patch test is now available for identification of allergens in aeroallergen-triggered atopic dermatitis. [1] Methods Seventy five subjects with atopic dermatitis fitting Hanifin and Rajka′s criteria and elevated serum IgE were included in the study. Patients with active disease who had taken drugs like antihistamines during the last 1week, corticosteroids [2] systemically during the last 4 weeks and topically during the last 1 week or who were on immunomodulators-topical and oral, [3] beta blockers or tricyclic antidepressants or who had dermatitis over the test site or were pregnant were excluded from the study. Personal and family history of atopic disorder was sought. Patch testing was done using prick test allergens in aluminium patch test chambers. The antigens are loaded in aluminium patch test chambers with filter paper using the dropper provided by the manufacturer. A drop from the dropper was approximately 1/16 ml. The test site was upper back. The antigens used were dust mites: D. farinae, D. pteronyssinus , [4] pollens of Cynodon dactylon and Parthenium hysterophorus , foods like rice, wheat, milk, egg and dog and cat epithelia. The reading was taken after 48 and 72 hours and interpretation and Grading of APT reaction was done according to the guidelines by European task force on atopic dermatitis consensus [Table - 1]. [5] Test material The patch test solutions were aqueous allergens supplied by Creative Drug Industries (Allergology division, Navi Mumbai) containing 50% glycerine as stabilizing factor and preserved with 0.4% phenol with their strengths expressed in protein nitrogen units (PNU) and for food series expressed in weight by volume. Dust mites i.e. Dermatophagoides farinae and D. pteronyssinus has 1500 PNU, all others ( Cynodon dactylon, Parthenium hysterophorus , dog and cat dander) has 5000 PNU. All food antigens have 1% weight by volume (w/v). Aluminium patch test chamber was supplied by Systopic Laboratories, New Delhi. Results Out of 75 subjects, 38 were males (51%) and 37 were females (49%) with mean age of 17.70 (1 to 64) years. Most of our study group belonged to the age group of 1 to 10 years [Figure - 1]. Seventy per cent of the subjects gave a personal or family history of an atopic disorder [Figure - 2]. The commonest site of involvement was cubital fossa followed by popliteal fossa [Figure - 3]. Out of the 75 subjects tested 46.66% (35) showed positive reactions, 50.66% (38) had no reaction [Figure - 4] and 2.66% (2) manifested angry back syndrome. While 28 subjects showed reaction to 1 antigen, 8 subjects showed reactions to 2 antigens. Parthenium accounted for 42.8%(15) of all positive reactions followed by Cynodon 20%(7), D. farinae 14%(5), D. pteronyssinus 11%(4), Milk 9%(3) and 6%(2) each to wheat, egg, dog dander and cat dander and only one subject reacted to rice - 3%. [Figure - 5]. Interestingly, among 15 parthenium APT positive subjects, 8 subjects were tested with the Indian Standard Series (ISS) and of these 6 subjects showed positive reaction to parthenium in ISS (delayed hypersensitivity). Discussion Recent studies show that there is a marked rise in the incidence and prevalence of atopic dermatitis in India. In India, the prevalence of atopic dermatitis ranges between 10 - 15.6%. [6] Atopic dermatitis can be diagnosed with Hanifin and Rajka′s criteria. Kanwar and Handa had undertaken a study to validate Hanifin and Rajka′s criteria and to assess the comparative efficacy of their criteria and the UK working party′s diagnostic criteria in the diagnosis of atopic dermatitis in a hospital setting in North India. Hanifin and Rajka′s criteria [sensitivity 96%, specificity 93.75%, positive predictive value 97% (PPV) and negative predictive value (NPV) 91.84%] had a statistical advantage over the UK working party′s diagnostic criteria (sensitivity 86%, specificity 95.83%, PPV 97.75% and NPV 76.67%), with a P -value < 0.005. [7] The correlation between the APT and the total and specific serum IgE suggests an important role for IgE in the reaction mechanism behind the APT. [8] Hence, we included only those subjects who had elevated total serum IgE. Dust mites are considered to be the most important triggering agent for atopic dermatitis. [9] In a study conducted in Croatia by Kuljanac et al, on Dermatophagoides pteronyssinus with APT and concluded that APT may detect the trigger factor in atopic dermatitis patients. [10] Cow milk and hen egg allergy are the most important food allergies in atopic dermatitis, [11],[12] avoidance resulted in the clinical improvement. Parthenium hysterophorus is the most important antigen in India with both type I and type IV hypersensitivity. [13] Both types I and IV hypersensitivity may play a role in parthenium associated atopic dermatitis as evidenced by reaction to both atopic patch test and to Indian standard series patch test. [13] Cynodon dactylon , also called Bermuda grass, has the potency of triggering atopic dermatitis. [14] Pet dander especially cat and dog dander should also be considered. [14] A study conducted in Germany regarding pre-treatment of atopic dermatitis with pimecrolimus cream concluded that APT can be used as a model for atopic dermatitis skin inflammation. [3] Pimecrolimus pre-treatment has a potential to suppress the development of lesions induced by aeroallergen exposure in patients with atopic dermatitis. [3] The atopic patch test (APT) involves the epicutaneous application of intact protein allergens in a diagnostic patch test setting with an evaluation of the induced eczematous skin lesions after 48 and 72 hours. The APT targets the cellular component of atopic dermatitis and helps complete out the atopic dermatitis test spectrum. As a number of apparently minor test modifications greatly influence the sensitivity, specificity, and reproducibility of the APT, the European Task Force on Atopic Dermatitis (ETFAD) has developed a standardized APT technique. [15] Aeroallergens and food allergens are able to elicit eczematous skin reactions after epicutaneous application. [16] Presence of at least seven papules after 72 h was the APT skin sign with the greatest diagnostic accuracy for food allergy in children with atopic dermatitis. [16] Counselling on avoidance of allergen based on APT can reduce the morbidity and can reduce the drug load. Immunotherapy for aeroallergens can be considered. Advantages of APT over skin prick tests are that: it can be tested at a younger age, risk of anaphylaxis is low and the specificity is high. Disadvantages are sensitivity is lower than SPT, it is time consuming and only a few antigens can be tested at a time. To date, no "gold standard" exists for the provocation of reactions in aeroallergen triggered atopic dermatitis and APT has not been standardised. Further analysis and comparison with skin prick testing and RAST should be done in a controlled study. The relevance of allergens for atopic dermatitis flares may be evaluated by APT in addition to skin prick test. Both immediate and delayed hypersensitivity may play a role in parthenium associated atopic dermatitis. Counselling based on patch test reports may help to reduce morbidity and improve quality of life. In our study, parthenium was found to be the commonest allergen in Bangalore. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08201f4.jpg] [dv08201t1.jpg] [dv08201f3.jpg] [dv08201f2.jpg] [dv08201f5.jpg] [dv08201f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}