 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
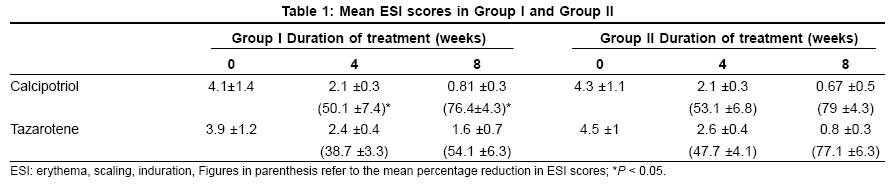
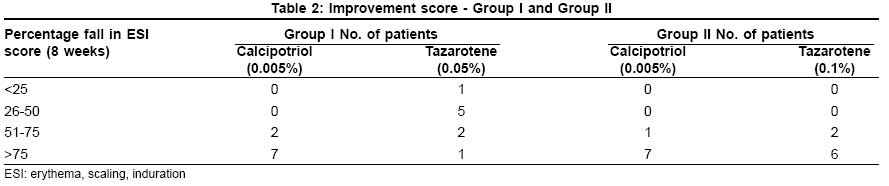
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 471-474 Brief Report Comparative study of calcipotriol (0.005%) ointment and tazarotene (0.05% and 0.1%) gel in the treatment of stable plaque psoriasis Kaur Inderjeet, Dogra Sunil, Jain Rajesh, Kumar Bhushan Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh Code Number: dv08202 Abstract Background: Topical therapies are the first line of treatment for patients with stable plaque psoriasis affecting a limited body surface area. Though in use for more than a decade, we could not find any reports of studies directly comparing calcipotriol and tazarotene.Aim: To evaluate the comparative efficacy and tolerability of calcipotriol and tazarotene in the treatment of stable plaque psoriasis. Methods: This was a prospective, right-left side intra-individual parallel 8-week study using calcipotriol 0.005% ointment applied twice daily (right side) versus tazarotene (left side) randomized to either 0.05% (group I) or 0.1% gel (group II) once daily in two groups, each of 10 patients. Efficacy was determined by the assessment of target psoriatic lesions under evaluation by using the severity scale (0-3) of erythema, scaling, and infiltration (ESI score). Evaluation was done at baseline (0 week), 4 weeks, and 8 weeks of treatment. At the end of 8 weeks, patients with more than 75% reduction in ESI score were considered to have marked improvement; 51% to 75%, moderate improvement; 26% to 50%, minimal improvement; and less than 25%, non-responders. Results: Seventeen patients (9 in group I, 8 in group II) completed the study. In group I, reduction in ESI score was significantly more at both 4 and 8 weeks on sides treated with calcipotriol, producing moderate-to-marked improvement (P < 0.05). In group II, improvement was comparable in lesions treated with either calcipotriol or tazarotene (0.1%) at the end of 4 and 8 weeks. Adverse effects noted were mild - in the form of burning, pruritus, and irritation - and were observed more often in the lesions treated with tazarotene as compared to those in the lesions treated with calcipotriol, but the difference was not statistically significant. However, none of the patients discontinued the therapy because of adverse events. Conclusion: Topical calcipotriol 0.005% ointment is more effective than tazarotene 0.05% gel; however, its efficacy is comparable to tazarotene 0.1% gel in the treatment of stable plaque psoriasis. Keywords: Calcipotriol, Psoriasis, Tazarotene Introduction Psoriasis is a common, genetically determined inflammatory and hyperproliferative skin disease with worldwide prevalence of 1% to 3%. [1] Although no cure is available, the disease can be effectively controlled by various therapeutic options, used alone or in combination. [2],[3] Topical therapies are the first line of treatment for patients with stable plaque psoriasis affecting a limited body surface area. Calcipotriol and tazarotene are newer topical treatment modalities in use since more than a decade in stable plaque psoriasis. Though there are studies comparing their effectiveness in psoriasis with that of various conventional topical treatments (coal tar, topical steroids, anthralin), [4],[5],[6],[7],[8],[9],[10] we could not find any reports of studies directly comparing calcipotriol and tazarotene used as monotherapies. The present study was planned to evaluate the comparative efficacy and tolerability of these two agents in the treatment of stable plaque psoriasis.Methods Twenty adult patients (12 males, 8 females) of mean age 31.7 ± 3 years (range, 18-44 years) having nearly bilateral symmetrical lesions of stable plaque psoriasis (SPP) on limbs involving a total surface area of not more than 100 cm 2 were recruited. This was a prospective intra-individual right-left comparative pilot study of 8 weeks′ duration using calcipotriol 0.005% ointment applied twice daily versus tazarotene randomized to either 0.05% or 0.1% gel once daily in two groups, each of 10 patients. In group I, calcipotriol 0.005% ointment was applied twice daily over lesions on the right side and tazarotene 0.05% once daily over lesions on the left side. In group II, calcipotriol 0.005% applied over lesions on the right side was compared with 0.1% tazarotene applied over lesions on the left side, with frequency of application remaining the same. All prior medications except antihistamines were stopped 4 weeks before the start of the study, and only application of an emollient (coconut oil) was permitted on both the sides. Serum calcium and phosphate estimation was done before and after therapy. The assessment of target psoriatic lesions under evaluation and progress during treatment were done using the erythema, scaling, and induration (ESI) score. The lesions were assessed on a grade from 0 to 3, i.e., 0 (nil), 1+ (mild), 2+ (moderate), and 3+ (severe); and a multiplication factor of 4 was applied to each grade. Thus the score ranged from 0 to 36. [11],[12] Evaluation was done at baseline (0 week) and at 4 and 8 weeks of treatment. The scores obtained were statistically compared using Wilcoxon test, and paired t test was used for comparing quantitative values. At the end of 8 weeks, patients with more than 75% reduction in ESI score were considered to have marked improvement; 51% to 75%, moderate improvement; 26% to 50%, minimal improvement; and less than 25%, no response.Results Seventeen patients (9 in group I, 8 in group II) completed the study. In group I, the reduction in ESI score was significantly more at both 4 and 8 weeks in the lesions treated with calcipotriol, resulting in moderate-to-marked improvement ( P < 0.05) [Table - 1]. At 8 weeks, all 9 patients treated with calcipotriol had more than 50% reduction (moderate improvement in 2, marked in 7) in ESI score as compared to only 3 patients treated with tazarotene ( P < 0.05) [Table - 2]. In group II, at the end of 4 weeks of treatment, both calcipotriol- and tazarotene-treated lesions showed similar reduction in scaling and infiltration in all patients. Reduction in erythema was more with calcipotriol, but there was no statistically significant change in the ESI score of the two groups as compared to baseline score ( P > 0.5). At the end of 8 weeks, improvement continued and was comparable in lesions treated with either calcipotriol or 0.1% tazarotene [Table - 1] All patients achieved moderate-to-marked improvement at the end of 8 weeks [Table - 2]. Adverse effects noted were mild in the form of burning, pruritus, and irritation and were observed more often in the lesions treated with tazarotene (0.1%) as compared to those in the lesions treated with calcipotriol, but the difference was not statistically significant. However, none of the patients discontinued the therapy because of adverse events. No alteration in serum calcium and phosphorus was observed during the study period. Discussion Calcipotriol (0.005%), a vitamin D3 analog, acts in psoriasis by inhibiting keratinocyte proliferation, inducing cellular differentiation and anti-inflammatory action. In various clinical trials, it was shown to be comparable to or slightly better than class II corticosteroid ointments such as fluocinonide 0.05%. [5] Compared with anthralin, it fared better in terms of clinical efficacy and was preferred by patients because it does not stain as much as anthralin and is less irritating. [6] Combination regimens in which patients apply both calcipotriol and superpotent corticosteroids (weekends-only) have demonstrated superiority over the regimen with either agent alone. [7] Side effects reported have been lesional and perilesional irritation, occasional hyperpigmentation, and sometimes hypercalcemia. [13] Studies on numerous parameters of calcium metabolism have not revealed clinically significant changes in patients who apply less than 100 g per week of calcipotriol ointment. Hence calcipotriol is well tolerated and continues to be clinically effective with minimum adverse effects. [14],[15] It is currently used as monotherapy to treat mild disease; and in moderate-to-severe plaque psoriasis, in combination with other treatment modalities. Tazarotene is the first of a new generation of acetylenic retinoids developed for the topical treatment of psoriasis. It specifically binds to b and g subtypes of retinoic acid receptor (RAR). Tazarotene appears to modulate three major pathogenic factors in psoriasis: keratinocyte hyperproliferation, abnormal keratinocyte differentiation, and dermal and epidermal inflammatory infiltration. [2] Tazarotene is available in gel and cream formulation at 0.05% and 0.1% concentrations. Lebwohl et al, [8] compared once-daily 0.1% and 0.05% topical tazarotene versus twice-daily 0.05% fluocinonide in stable plaque psoriasis in 348 patients and found that tazarotene had a therapeutic effect similar to that of fluocinonide at 12 weeks of treatment; but tazarotene demonstrated significantly better maintenance of therapeutic effect after cessation of therapy. Schiener et al, [9] comparing the effect of combining narrow-band ultraviolet B irradiation with either topical tazarotene or topical calcipotriol in 10 patients each found significant improvement of psoriatic lesions after 4 weeks of therapy without any therapeutic difference between the two regimens. Like calcipotriol, side effects of corticosteroids, including atrophy, tachyphylaxis, and rebound are avoided with the use of tazarotene. Adverse effects reported with tazarotene are mild, including pruritus, burning/stinging, erythema, worsening of psoriasis, and irritation. They are most common during the first 1 to 2 weeks of therapy. Efforts have been undertaken to minimize the irritating nature of retinoids and enhance their action by combining topical corticosteroids. No serious systemic adverse effects were observed in clinical trials involving approximately 2000 patients treated with tazarotene (0.05%, 0.1%) gel for a period of 1 year. [16],[17],[18] Petrolatum, emollients, or barrier creams may be used on the skin around psoriatic plaques to protect it from irritation. The one with 0.1% concentration is most commonly used since it has enhanced efficacy over that with 0.05% concentration. Particularly in patients with sensitive skin who might be prone to irritation, it is recommended that treatment be initiated with the 0.05% formulation and stepped up as tolerated. Tazarotene is typically applied before bedtime. [19] There is no published report of directly comparing calcipotriol with tazarotene in plaque-type psoriasis. Guenther et al, [20] compared tazarotene 0.1% gel once daily plus mometasone furoate 0.1% cream once daily versus calcipotriene 0.005% ointment twice daily in the treatment of plaque psoriasis. At the end of the 12-week post-treatment period, significantly more tazarotene plus mometasone furoate recipients compared to the number of calcipotriol recipients rated their treatment as favorable or highly favorable (84% vs. 73%). Both tazarotene and calcipotriol as monotherapy or in combination with corticosteroids or UV therapy represent a useful treatment option in patients with plaque psoriasis. [21],[22] Topical calcipotriol 0.005% ointment seems to be more effective than tazarotene 0.05% gel; however, its efficacy is comparable to tazarotene 0.1% gel in the treatment of stable plaque psoriasis. Both calcipotriol and tazarotene are cosmetically acceptable, but the difference in cost is marked in resource-poor settings. However, small sample size is the main limitation of this trial, and it is necessary to conduct a larger study in blinded manner. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08202t1.jpg] [dv08202t2.jpg] |
| |||||||||

{kind=link}
{kind=link}