 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
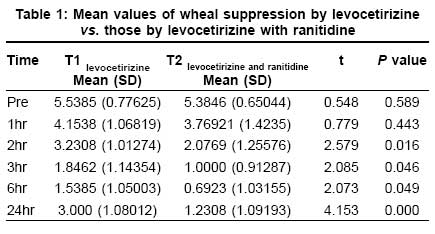
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 475-477 Brief Report Histamine 2 blocker potentiates the effects of histamine 1 blocker in suppressing histamine-induced wheal Dhanya NB, Rai Reena, Srinivas CR Department of Dermatology, PSG Hospitals, Coimbatore Code Number: dv08203 Abstract Background : Histamine is responsible for the wheal and flare reaction in various allergic conditions. Classical antihistamines are the drugs which block the H 1 receptors and are widely used in various allergic conditions, whereas H 2 blockers are mainly used for acid peptic disease. Although H 1 receptor-mediated actions of histamine are primarily responsible for vasodilatation, vasopermeability, and itching, it has been observed that combined blocking of both H 1 and H 2 receptors may provide better relief. Keywords: Histamine1 blocker, Histamine 2 blocker, Histamine-induced wheal Introduction Histamine is a major mediator in allergic reactions. It is secreted as a result of the interaction of antigens with IgE antibodies on mast cells and results in profound pharmacological effects, both locally and systemically. [1] Four histamine receptors have been identified. H 1 and H 2 receptors are found in cutaneous blood vessels, and H 3 receptors are located in the brain. [2] The function of the H4 receptor is not known. Activation of either H1 or H2 receptors increases vasodilation of vascular endothelium and elicits negative ionotropic effects on myocytes through release of nitric oxide. Nitric oxide-mediated vasodilation through the H1 receptors plays a part in the flare reaction. The action of histamine on bronchial smooth muscle and blood vessels accounts in part for allergic symptoms (H1 and H2 receptors). It also has a major role in regulation of gastric secretions by inducing acid and peptin secretion (H2 receptors), formation of edema (wheal and flare), and stimulation of sensory nerve endings (H1 and H2). [1] Classical antihistamines are the drugs which block the H 1 receptors and are widely used in various allergic conditions, whereas H 2 blockers are mainly used for acid peptic disease. Although H 1 receptor-mediated actions of histamine are primarily responsible for vasodilatation, vasopermeability, and itching, it has been observed that combined blocking of both H 1 and H 2 receptors may provide better relief. [3] Based on this, we conducted a study to compare the efficacy of levocetirizine (H 1 blocker) versus levocetirizine and ranitidine (H 2 blocker) in suppressing histamine-induced wheal. Methods The study was done on 15 healthy volunteers (10 males and 5 females) in the age group of 18 to 50 years after obtaining informed consent. The volunteers were not on antihistamines, steroid, and immunosuppressants for 7 days prior to the study. None of them had history of atopy, drug hypersensitivity, or use of alcohol. Pregnant and lactating women were excluded. Volunteers were administered a single dose of levocetirizine 5 mg on day 1 and a single dose of levocetirizine 5 mg with ranitidine 150 mg twice a day on day 7. Ranitidine 150 mg was given twice a day because it is the recommended dose . A prick test was performed before administration of the drugs by the standard method using histamine 0.1% w/v solution. A drop of 0.1% w/v of histamine solution was placed on the flexor aspect of the forearm. The skin was pricked through the histamine solution with a lancet. The tip of the lancet was kept parallel to the skin surface and the skin lifted by tenting the lancet by 45° to 60°. After 1 minute, the test site was wiped with filter paper to remove the excess histamine solution. The size of wheal was calculated by measuring the maximum diameter of the wheal and the orthogonal diameter with a transparent scale. Multiple squares of size 1x1 cm were marked on the flexor aspect of the forearm. The prick test was repeated within the squares at 1 hour, 2, 3, 6, and 24 hours after administering the drug on day 1 and day 7. The size of the histamine-induced wheal was recorded each time. Results The mean values of wheal size in response to intradermal histamine challenge for levocetirizine and for levocetirizine with ranitidine at 1 hour, 2, 3, 6, and 24 hours were analyzed using SPSS PC 11.5 version. Mean and standard deviations were computed. Paired t test was used to compare the mean values. P value < 0.05 was considered statistically significant. At 1 hour, there was no statistically significant difference in the wheal size between levocetirizine alone and combination of levocetirizine and ranitidine. Levocetirizine with ranitidine resulted in statistically significant reduction of wheal size at 2, 3, 6, and 24 hours when compared with levocetirizine alone [Table - 1]. Discussion Levocetirizine is an active enantiomer of cetirizine, which is a widely used H 1 blocker for allergic conditions; whereas ranitidine is an H2 blocker used in acid peptic disease. Studies have shown that the combination of chlorpheniramine (H 1 antagonist) and cimetidine (H 2 antagonist) is more successful in inhibiting a histamine skin reaction when compared with an H 1 antagonist alone, and it is recommended for the treatment of chronic idiopathic urticaria. [4] Other studies using cetirizine and ranitidine, diphenhydramine and ranitidine, terfenadine and ranitidine showed similar results. [5],[6],[7] The results provided additional evidence that H2 receptors are present in the human cutaneous microcirculation and add support to the clinical observation of therapeutic efficacy of H 1 plus H 2 blockers in some patients with chronic urticaria. [8],[9] It has been suggested that the H 1 antagonist-H 2 antagonist combination inhibits the release of allergic mediators, whether IgE dependent or otherwise. [10],[11],[12] Another view suggests that the response to the combination may be highly individual and that there could be a subpopulation of urticaria patients whose response to it is especially favorable. [13],[14] In our study, we found that the wheal suppression started at the end of 2 hours and lasted till the end of 24 hours. Urticaria may sometimes be resistant to treatment by H1 blocker and so an H2 blocker may potentiate the effects of an H1 blocker. [15] There are also increasing reports of the beneficial effects of H 2 -antagonists, mostly in combination with H 1 -antagonists, in a variety of allergic and pseudoallergic conditions such as chronic urticaria and anaphylactoid reactions due to colloid volume substitutes, opioid analgesics, and radiographic contrast media. The combined use of H 1 - and H 2 -antagonists might not only act as specific histamine antagonism but also exert a mast cell stabilizing effect, as demonstrated in animal experiments and some clinical studies. [16] These results support the rationale of using the combination of H1- and H2-antagonists in urticarial disease not responding to H1 blockers alone. Future research may show whether the combined use of H 1 - and H 2 -antagonists will become a routine therapeutic procedure in allergy therapy. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08203t1.jpg] |
| |||||||||

{kind=link}