 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
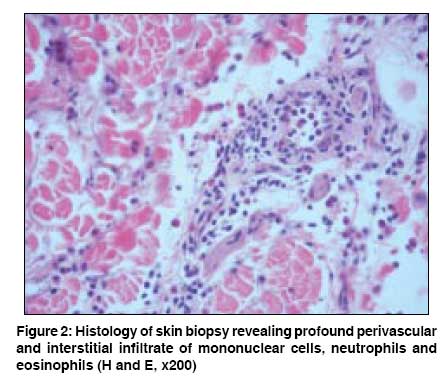
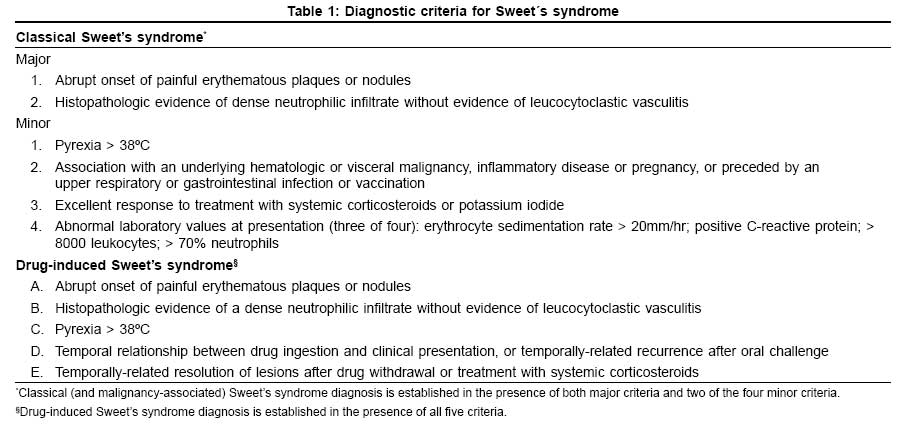
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 478-480 Case Report Neutrophilic dermatosis of the dorsal hands associated with chronic hepatitis C virus infection Coelho JoaoFigueira, Lourenco Sofia, Marques Joana, Mendonca Paula, Malhado JoseAntonio Unit of Internal Medicine I - Hospital Curry Cabral, Lisbon Code Number: dv08204 Abstract Neutrophilic dermatosis of the dorsal hands, a localized form of Sweet's syndrome, was recently described, and can be associated with several diseases including infections. Chronic hepatitis C virus infection has been proposed as a possible triggering factor. The authors present a case in which the clinical and laboratory workup diagnosis only revealed positive serology for hepatitis C virus. Although a cause-effect relation could not be proved, it might be advisable to include serology for this virus in the initial evaluation of patients with neutrophilic dermatosis.Keywords: Hepatitis C virus, Neutrophilic dermatosis of the dorsal hands, Sweet′s syndrome Introduction Neutrophilic dermatosis of the dorsal hands (NDDH) has been recently described as a form of Sweet′s syndrome which can be associated with cancer, inflammatory bowel disease, drugs, pregnancy, and infections. Several dermatologic diseases have been recognized in chronic hepatitis C virus infection and this agent has been suggested as a possible triggering factor for neutrophilic dermatosis.Case Report A 37 year-old male, born in Georgia, a bus driver, with no past medical history, including personal or familiar history of atopic diseases, arrived at our Emergency Room with a 3 hours course of fever (38.4°C) and progressive edema of the hands with painful erythematous plaques and intertriginous hemorrhagic bullae [Figure - 1]. He denied taking any medication, and any direct contact with animals or chemical products. His cardiac and pulmonary auscultation was normal; the abdomen was soft and no hepatomegaly or splenomegaly was present. He had no palpable lymphadenopathy and the oropharynx was normal. Laboratory workup results showed leukocytosis (14.900x10 9 /L) with neutrophilia (82.5%), C-reactive protein=3.2mg/dL, erythrocyte sedimentation rate=14mm/hr, creatine kinase=195U/L. Liver enzymes, renal and thyroid function, and urinalysis were normal. The autoimmune study (ANA, Anti-dsDNA, cANCA, pANCA, C3, C4) was negative, including anti-skin antibodies (anti-intercellular and anti-basement membrane). Serology for Hepatitis C virus was positive. Other viruses, namely Hepatitis B virus, HIV 1 and 2, Epstein Barr virus, Herpes virus 1 and 2 and Parvovirus B19 were negative. Blood cultures and VDRL were negative, as well. On the second day, the patient remained febrile and developed erythematous plaques on the internal face of both arms and legs, along with edema and erythema on both feet. A skin biopsy of the arm lesions revealed profound dermal inflammatory infiltrate, perivascular and interstitial, by mononuclear cells, neutrophils and eosinophils, compatible with Sweet′s syndrome [Figure - 2]. The patient was begun on oral prednisolone 60mg/day and fever responded promptly. After a week of steroid therapy the skin lesions had almost completely cleared with no scarring, and he was discharged on a tapering dose of prednisolone. Discussion Sweet′s syndrome, also known as acute febrile neutrophilic dermatosis, was first described by Dr. Robert Douglas Sweet in 1964. Classified as classic or idiopathic, malignancy-associated and drug-induced, it is characterized by the presence of painful erythematous plaques or nodules on the skin, associated with fever and leukocytosis, with an excellent response to corticosteroid treatment. [1] In 1995, Strutton described six women with erythematous plaques, pustules and hemorrhagic bullae limited to the dorsa of the hands, fulfilling Sweet′s syndrome criteria except for the fact that the skin biopsy revealed vasculitis [Table - 1]. He, then, proposed the term pustular vasculitis of the hands. [2] In 2000, Galaria revisited this entity and suggested the term neutrophilic dermatosis of the dorsal hands for 3 patients with similar symptoms but lacking systemic involvement and vasculitis in biopsy specimens, considering it a subset of Sweet′s syndrome [3] Several cases have been described since then and a review of 52 reported cases of NDDH made by Walling in 2006, supported the idea that this entity is strongly related to Sweet′s syndrome, representing a distributional variant form. Most of the patients were female, showed fever, peripheral neutrophilia and leukocytosis; they responded to systemic corticosteroid therapy and the association with hematologic diseases and bowel inflammatory disease was present in some patients. The presence or absence of vasculitis does not appear to be essential for the diagnosis of NDDH. Its presence in NDDH and in Sweet′s syndrome does not seem to be the trigger for the disease but the result of the inflammatory neutrophilic infiltrate, correlating positively with the duration of the disease at the time the biopsy is made. [4] Several infectious agents have been associated with Sweet′s syndrome, namely and in order of frequency reported in the literature, Streptococcus pneumoniae , Yersinia enterocolitica , Mycobacterium tuberculosis , Cytomegalovirus, Hepatitis B virus, HIV, Salmonella enteritidis , Salmonella typhimurium , Coccidioides immitis , Helicobacter pylori , Chlamydia pneumoniae , Staphylococcus aureus , Escherichia coli and Toxoplasma spp. [5] Hepatitis C virus is known to be associated with several extra-hepatic manifestations, including dermatologic diseases like mixed cryoglobulinemia, porphyria cutanea tarda, lichen planus, erythema nodosum, malakoplakia, urticaria, erythema multiforme, pruritus, pyoderma gangrenosum and polyarteritis nodosa. [6] The pathogenic mechanism of several of these identified associations is yet to be explained. In 2003, Baz et al. suggested that hepatitis C virus might be a triggering factor for Sweet′s syndrome. [7] Our patient did not show clinical and/or laboratory features for other possible conditions associated with NDDH / Sweet′s Syndrome. The serology for hepatitis C virus was positive and a possible association cannot be ruled out, although we cannot explain its pathogenic mechanism. One possible hypothesis is that an eventual rise of serum hepatitis C virus-RNA level in our patient could have been the trigger for NDDH. The hepatitis C virus-RNA levels are known to fluctuate in untreated patients with chronic hepatitis C infection, without obligatory correlation with transaminases levels. [8] Furthermore, T-helper 1 inflammatory cells, characterized by interferon (IFN)-gamma and interleukin (IL)-2 secretion, predominate in the liver during chronic hepatitis C virus infection [9] and the pathogenesis of neutrophilic dermatosis, although not completely understood, seems to be an immunological reactive response to a viral, bacterial or tumoral antigen, also probably mediated by T-helper 1 cells, as evidenced by elevated serum INF-gamma and IL-2 in patients with Sweet Syndrome. [10] We propose the inclusion of serology for hepatitis C virus in the initial workup diagnosis of more cases of NDDH / Sweet′s syndrome in order to evaluate if this association is frequent and consistent. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08204f2.jpg] [dv08204f1.jpg] [dv08204t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}